van der Staaij Hilde, Donker Albertine E, Bakkeren Dirk L, Salemans Jan M J I, Mignot-Evers Lisette A A, Bongers Marlies Y, Dieleman Jeanne P, Galesloot Tessel E, Laarakkers Coby M, Klaver Siem M, Swinkels Dorine W
Translational Metabolic Laboratory, Department of Laboratory Medicine, Radboud University Medical Center (Radboudumc), 6525 GA Nijmegen, The Netherlands.
Máxima Medical Center (MMC), Department of Pediatrics, 5504 DB Veldhoven, The Netherlands.
Int J Mol Sci. 2022 Feb 8;23(3):1917. doi: 10.3390/ijms23031917.
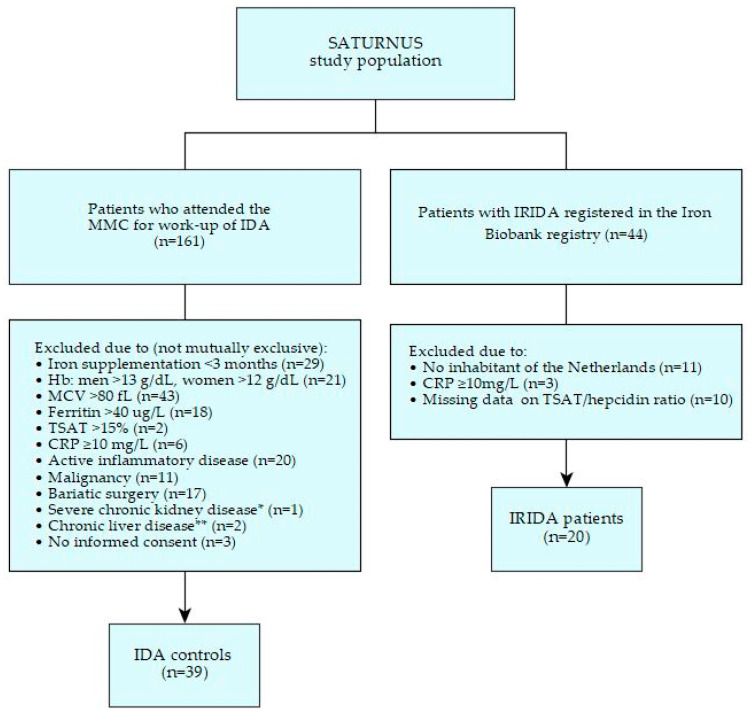
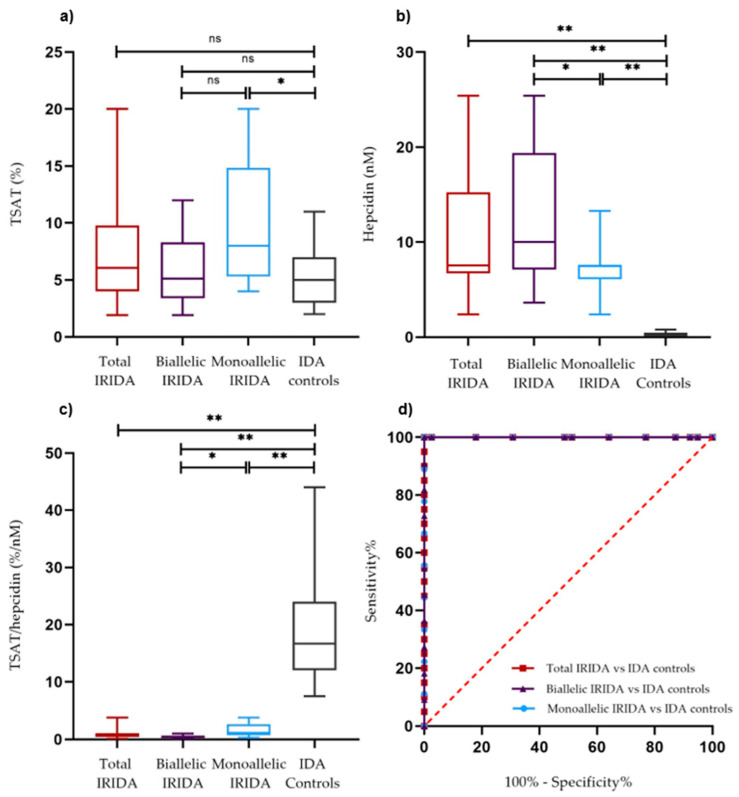
Pathogenic variants impairing matriptase-2 function result in inappropriately high hepcidin levels relative to body iron status, leading to iron refractory iron deficiency anemia (IRIDA). As diagnosing IRIDA can be challenging due to its genotypical and phenotypical heterogeneity, we assessed the transferrin saturation (TSAT)/hepcidin ratio to distinguish IRIDA from multi-causal iron deficiency anemia (IDA). We included 20 IRIDA patients from a registry for rare inherited iron disorders and then enrolled 39 controls with IDA due to other causes. Plasma hepcidin-25 levels were measured by standardized isotope dilution mass spectrometry. IDA controls had not received iron therapy in the last 3 months and C-reactive protein levels were <10.0 mg/L. IRIDA patients had significantly lower TSAT/hepcidin ratios compared to IDA controls, median 0.6%/nM (interquartile range, IQR, 0.4-1.1%/nM) and 16.7%/nM (IQR, 12.0-24.0%/nM), respectively. The area under the curve for the TSAT/hepcidin ratio was 1.000 with 100% sensitivity and specificity (95% confidence intervals 84-100% and 91-100%, respectively) at an optimal cut-off point of 5.6%/nM. The TSAT/hepcidin ratio shows excellent performance in discriminating IRIDA from -unrelated IDA early in the diagnostic work-up of IDA provided that recent iron therapy and moderate-to-severe inflammation are absent. These observations warrant further exploration in a broader IDA population.
损害matriptase-2功能的致病性变异会导致相对于机体铁状态而言,铁调素水平异常升高,从而引发铁难治性缺铁性贫血(IRIDA)。由于IRIDA具有基因型和表型异质性,其诊断可能具有挑战性,因此我们评估了转铁蛋白饱和度(TSAT)/铁调素比值,以区分IRIDA和多病因缺铁性贫血(IDA)。我们纳入了一个罕见遗传性铁紊乱登记处的20例IRIDA患者,然后招募了39例因其他原因患IDA的对照者。采用标准化同位素稀释质谱法测定血浆铁调素-25水平。IDA对照者在过去3个月内未接受铁治疗,且C反应蛋白水平<10.0 mg/L。与IDA对照者相比,IRIDA患者的TSAT/铁调素比值显著更低,中位数分别为0.6%/nM(四分位间距,IQR,0.4 - 1.1%/nM)和16.7%/nM(IQR, 12.0 - 24.0%/nM)。在最佳切点为5.6%/nM时,TSAT/铁调素比值的曲线下面积为1.000,敏感性和特异性均为100%(95%置信区间分别为84 - 100%和91 - 100%)。在IDA的诊断工作早期,若不存在近期铁治疗及中度至重度炎症,TSAT/铁调素比值在区分IRIDA和无关的IDA方面表现优异。这些观察结果值得在更广泛的IDA人群中进一步探索。