Medicine, Division of General Internal Medicine, University of California San Francisco, 1001 Potrero Avenue, San Francisco, CA, 94110, USA.
Center for Vulnerable Populations, Zuckerberg San Francisco General Hospital and Trauma Center, San Francisco, CA, USA.
BMC Health Serv Res. 2022 Feb 14;22(1):195. doi: 10.1186/s12913-022-07547-9.
The COVID-19 pandemic triggered unprecedented expansion of outpatient telemedicine in the United States in all types of health systems, including safety-net health systems. These systems generally serve low-income, racially/ethnically/linguistically diverse patients, many of whom face barriers to digital health access. These patients' perspectives are vital to inform ongoing, equitable implementation efforts.
Twenty-five semi-structured interviews exploring a theoretical framework of technology acceptability were conducted from March through July 2020. Participants had preferred languages of English, Spanish, or Cantonese and were recruited from three clinics (general medicine, obstetrics, and pulmonary) within the San Francisco Health Network. Both deductive and inductive coding were performed. In a secondary analysis, qualitative data were merged with survey data to relate perspectives to demographic factors and technology access/use.
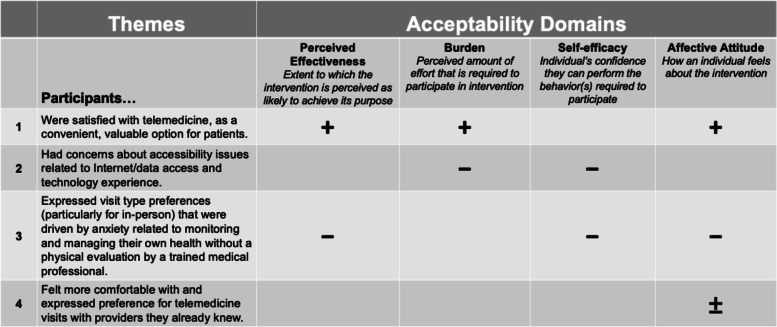
Participants were diverse with respect to language (52% non-English-speaking), age (range 23-71), race/ethnicity (24% Asian, 20% Black, 44% Hispanic/Latinx, 12% White), & smartphone use (80% daily, 20% weekly or less). All but 2 had a recent telemedicine visit (83% telephone). Qualitative results revealed that most participants felt telemedicine visits fulfilled their medical needs, were convenient, and were satisfied with their telemedicine care. However, most still preferred in-person visits, expressing concern that tele-visits relied on patients' abilities to access telemedicine, as well as monitor and manage their own health without in-person physical evaluation.
High satisfaction with telemedicine can co-exist with patient-expressed hesitations surrounding the perceived effectiveness, self-efficacy, and digital access barriers associated with a new model of care. More research is needed to guide how healthcare systems and clinicians make decisions and communicate about visit modalities to support high-quality care that responds to patients' needs and circumstances.
COVID-19 大流行促使美国所有类型的医疗体系(包括安全网医疗体系)中的门诊远程医疗以前所未有的规模扩张。这些系统通常为低收入、种族/族裔/语言多样化的患者提供服务,其中许多人面临数字医疗获取障碍。这些患者的观点对于告知正在进行的公平实施工作至关重要。
2020 年 3 月至 7 月期间,进行了 25 次半结构化访谈,探讨了技术可接受性的理论框架。参与者的首选语言为英语、西班牙语或粤语,并从旧金山健康网络的三个诊所(普通医学、妇产科和肺病科)招募。进行了演绎和归纳编码。在二次分析中,将定性数据与调查数据合并,将观点与人口统计学因素和技术访问/使用相关联。
参与者在语言(52%非英语)、年龄(23-71 岁)、种族/族裔(24%亚洲人、20%黑人、44%西班牙裔/拉丁裔、12%白人)和智能手机使用(80%每天,20%每周或更少)方面存在差异。除了 2 人之外,所有人最近都进行了远程医疗访问(83%电话)。定性结果表明,大多数参与者认为远程医疗访问满足了他们的医疗需求,方便且对远程医疗护理感到满意。然而,大多数人仍然更喜欢亲自就诊,他们表示担心远程就诊依赖于患者访问远程医疗的能力,以及在没有亲自进行身体评估的情况下监测和管理自己健康的能力。
对远程医疗的高度满意可能与患者对新护理模式的有效性、自我效能和数字获取障碍的担忧并存。需要进一步研究,以指导医疗保健系统和临床医生如何就就诊方式做出决策并进行沟通,以支持满足患者需求和情况的高质量护理。