Victorian Heart Institute, Monash University, Melbourne, Vic, Australia; MonashHeart, Monash Health, Melbourne, Vic, Australia.
Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Vic, Australia; Data Science and Artificial Intelligence platform (DSAI), eResearch, Monash University, Melbourne, Vic, Australia.
Heart Lung Circ. 2022 Jun;31(6):787-794. doi: 10.1016/j.hlc.2021.10.019. Epub 2022 Feb 11.
Countries who suffered large COVID-19 outbreaks reported a decrease in acute coronary syndrome (ACS) presentations and percutaneous coronary intervention (PCI). The impact of the pandemic in countries like Australia, with relatively small outbreaks yet significant social restrictions, is relatively unknown. There is also limited and conflicting data regarding the impact on clinical outcomes, symptom-to-door time (STDT) and door-to-balloon time (DTBT).
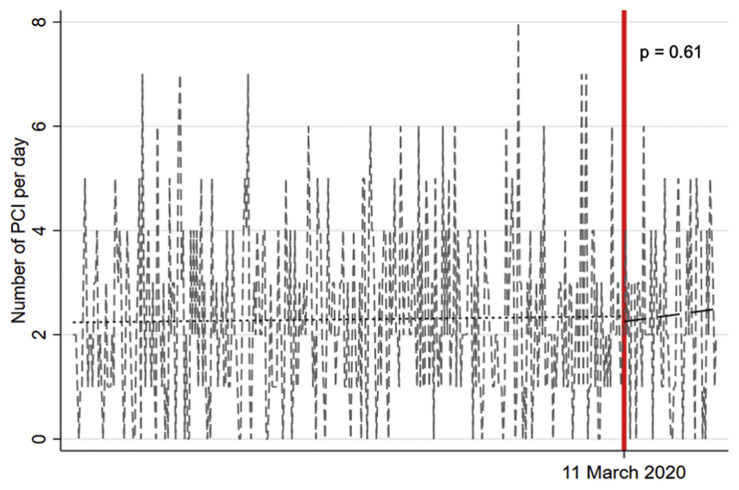
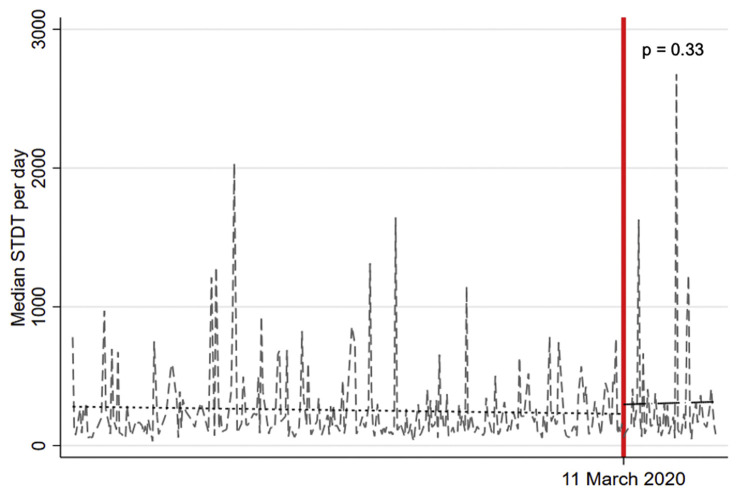
Consecutive ACS patients treated with PCI were prospectively recruited from a tertiary hospital network in Melbourne, Australia. The pre-pandemic period (11 March 2019-10 March 2020) was compared to the pandemic period (11 March 2020-10 May 2020) using an interrupted time series analysis with a primary endpoint of number PCI-treated ACS per day. Secondary endpoints included STDT, DTBT, total mortality and major adverse cardiac events (MACE).
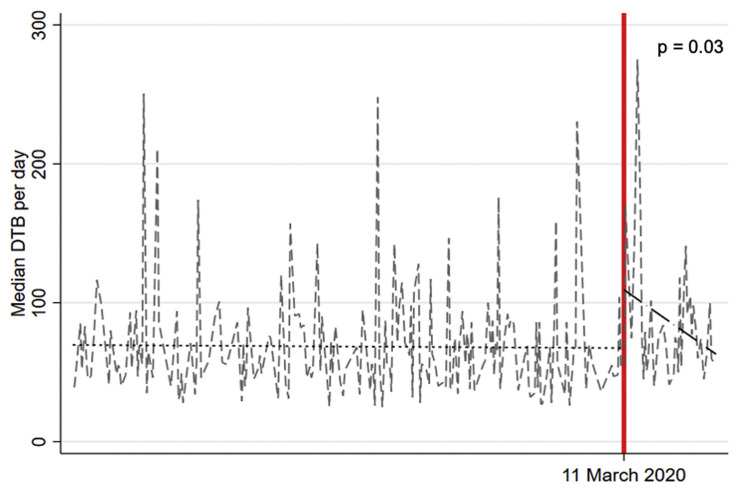
A total 984 ACS patients (14.8% during the pandemic period) received PCI. Mean number of PCI-treated ACS per day did not differ between the two periods (2.3 vs 2.4, p=0.61) with no difference in STDT [+51.3 mins, 95% confidence interval (CI) -52.4 to 154.9, p=0.33], 30-day mortality (5% vs 5.3%, p=0.86) or MACE (5.2% vs 6.1%, p=0.68). DTBT was significantly longer during the pandemic versus the pre-pandemic period (+18.1 mins, 95% CI 1.6-34.5, p=0.03) and improved with time (slope estimate: -0.76, 95% CI -1.62 to 0.10).
Despite significant social restrictions imposed in Melbourne, numbers of ACS treated with PCI and 30-day outcomes were similar to pre-pandemic times. DTBT was significantly longer during the COVID-19 pandemic period, likely reflecting infection control measures, which reassuringly improved with time.
遭受大规模 COVID-19 疫情的国家报告急性冠状动脉综合征 (ACS) 发作和经皮冠状动脉介入治疗 (PCI) 减少。在澳大利亚等国家,疫情相对较小但社会限制较大,其影响尚不清楚。关于对临床结果、症状至门时间 (STDT) 和门至球囊时间 (DTBT) 的影响,也存在有限的和相互矛盾的数据。
连续 ACS 患者在澳大利亚墨尔本的三级医院网络中前瞻性接受 PCI 治疗。使用中断时间序列分析比较大流行前时期 (2019 年 3 月 11 日至 2020 年 3 月 10 日) 和大流行时期 (2020 年 3 月 11 日至 2020 年 5 月 10 日),主要终点为每日接受 PCI 治疗的 ACS 数量。次要终点包括 STDT、DTBT、总死亡率和主要不良心脏事件 (MACE)。
共有 984 例 ACS 患者 (大流行期间占 14.8%) 接受了 PCI。两个时期的每日接受 PCI 治疗的 ACS 数量没有差异 (2.3 与 2.4,p=0.61),STDT 无差异 [+51.3 分钟,95%置信区间 (CI) -52.4 至 154.9,p=0.33],30 天死亡率 (5%与 5.3%,p=0.86) 或 MACE (5.2%与 6.1%,p=0.68)。与大流行前时期相比,大流行期间的 DTBT 明显延长 (+18.1 分钟,95% CI 1.6-34.5,p=0.03),且随时间推移而改善 (斜率估计值:-0.76,95% CI -1.62 至 0.10)。
尽管在墨尔本实施了重大社会限制,但接受 PCI 治疗的 ACS 数量和 30 天结局与大流行前时期相似。在 COVID-19 大流行期间,DTBT 明显延长,可能反映了感染控制措施,这些措施随时间推移而有所改善。