Fundação Oswaldo Ramos, Hospital do Rim, Unidade de Terapia Intensiva, São Paulo, SP, Brasil.
Fundação Oswaldo Ramos, Hospital do Rim, Departamento de Transplante, São Paulo, SP, Brasil.
J Bras Nefrol. 2022 Jul-Sep;44(3):383-394. doi: 10.1590/2175-8239-JBN-2021-0155.
the predictive ability of severity scores for mortality in patients admitted to intensive care units is not well-known among kidney transplanted (KT) patients, especially those diagnosed with coronavirus disease 2019 (COVID-19). The purpose of the present study was to evaluate the predictive ability of severity scores for mortality in KT recipients.
51 KT recipients with COVID-19 diagnosis were enrolled. The performance of the SOFA, SAPS 3, and APACHE IV tools in predicting mortality after COVID-19 was compared by the area under the ROC curve (AUC-ROC) and univariate Cox regression analysis was performed.
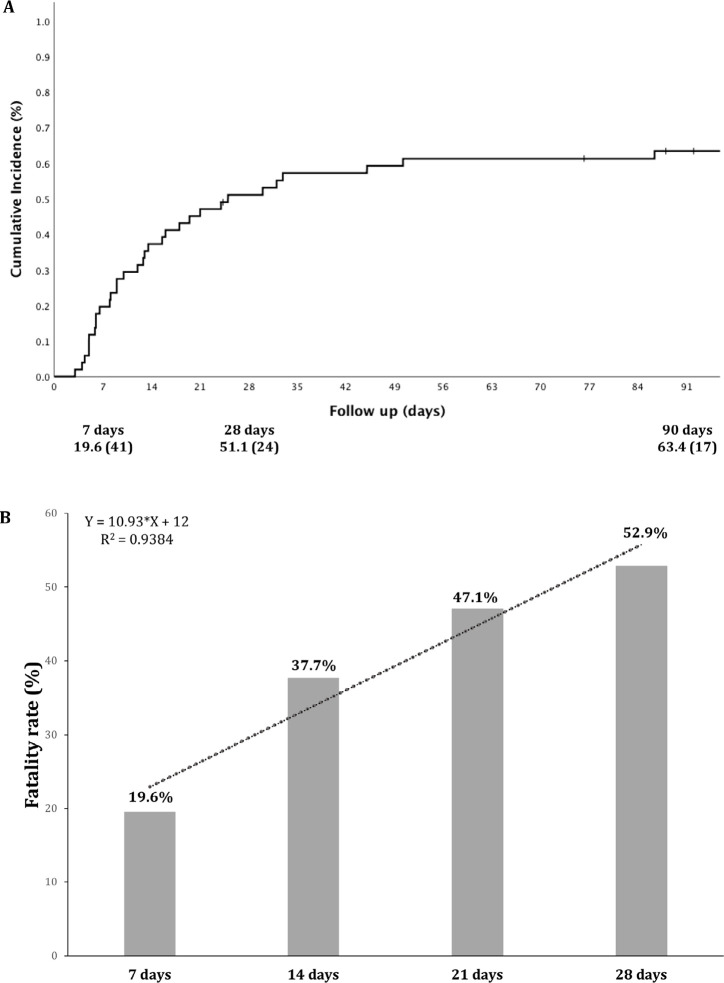
The 90-day cumulative incidence of death was 63.4%. Only APACHE IV score differed between survivors and nonsurvivors: 91.2±18.3 vs. 106.5±26.3, P = 0.03. The AUC- ROC of APACHE IV for predicting death was 0.706 (P = 0.04) and 0.656 (P = 0.06) at 7 and 90 days, respectively. Receiving a kidney from a deceased donor (HR = 3.16; P = 0.03), troponin levels at admission (HR for each ng/mL = 1.001; P = 0.03), APACHE IV score (HR for each 1 point = 1.02; P = 0.01), mechanical ventilation (MV) requirement (HR = 3.04; P = 0.002) and vasopressor use on the first day after ICU admission (HR = 3.85; P < 0.001) were associated with the 90-day mortality in the univariate analysis.
KT recipients had high mortality, which was associated with type of donor, troponin levels, early use of vasopressors, and MV requirement. The other traditional severity scores investigated could not predict mortality.
在重症监护病房接受治疗的肾移植(KT)患者中,严重程度评分对死亡率的预测能力尚不清楚,尤其是那些被诊断患有 2019 年冠状病毒病(COVID-19)的患者。本研究旨在评估严重程度评分对 KT 受者死亡率的预测能力。
纳入 51 例被诊断为 COVID-19 的 KT 患者。通过 ROC 曲线下面积(AUC-ROC)比较 SOFA、SAPS 3 和 APACHE IV 工具对 COVID-19 后死亡率的预测能力,并进行单因素 Cox 回归分析。
90 天累积死亡率为 63.4%。仅 APACHE IV 评分在幸存者和非幸存者之间存在差异:91.2±18.3 vs. 106.5±26.3,P=0.03。APACHE IV 预测死亡的 AUC-ROC 在 7 天和 90 天分别为 0.706(P=0.04)和 0.656(P=0.06)。接受已故供者的肾脏(HR=3.16;P=0.03)、入院时肌钙蛋白水平(每增加 1ng/mL 的 HR=1.001;P=0.03)、APACHE IV 评分(每增加 1 分的 HR=1.02;P=0.01)、机械通气(MV)需求(HR=3.04;P=0.002)和 ICU 入院后第一天使用升压药(HR=3.85;P<0.001)与 90 天死亡率的单因素分析相关。
KT 受者死亡率较高,与供者类型、肌钙蛋白水平、早期使用升压药和 MV 需求有关。研究中其他传统严重程度评分无法预测死亡率。