Faculty of Medicine, University of Southampton, Southampton, UK.
Faculty of Medicine, University of Southampton, Southampton, UK
BMJ Open. 2022 Feb 15;12(2):e050331. doi: 10.1136/bmjopen-2021-050331.
COVID-19 is a heterogeneous disease, and many reports have described variations in demographic, biochemical and clinical features at presentation influencing overall hospital mortality. However, there is little information regarding longitudinal changes in laboratory prognostic variables in relation to disease progression in hospitalised patients with COVID-19.
This retrospective observational report describes disease progression from symptom onset, to admission to hospital, clinical response and discharge/death among patients with COVID-19 at a tertiary centre in South East England.
Six hundred and fifty-one patients treated for SARS-CoV-2 between March and September 2020 were included in this analysis. Ethical approval was obtained from the HRA Specific Review Board (REC 20/HRA/2986) for waiver of informed consent.
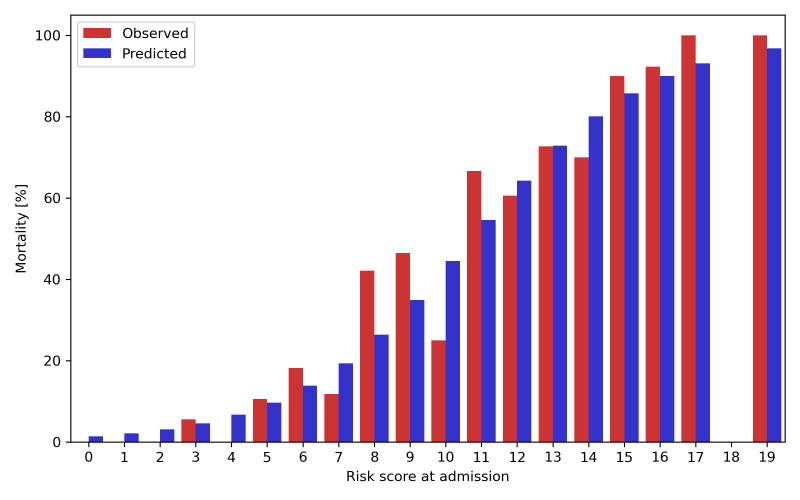
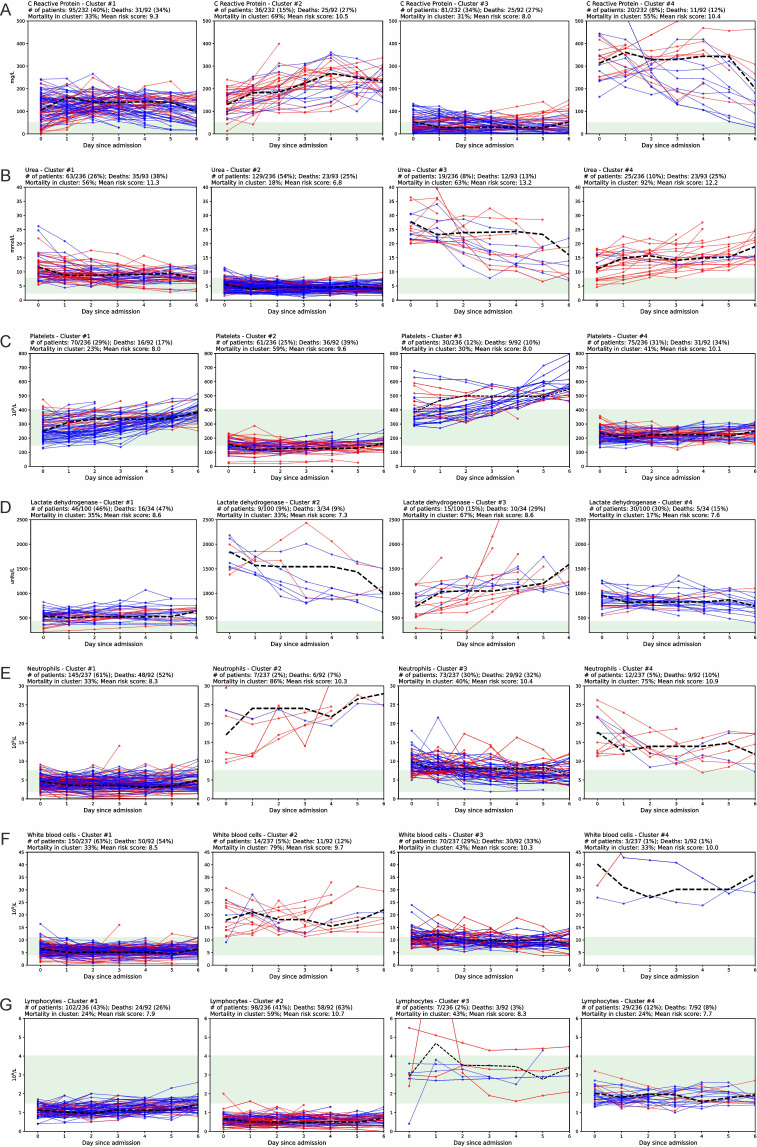
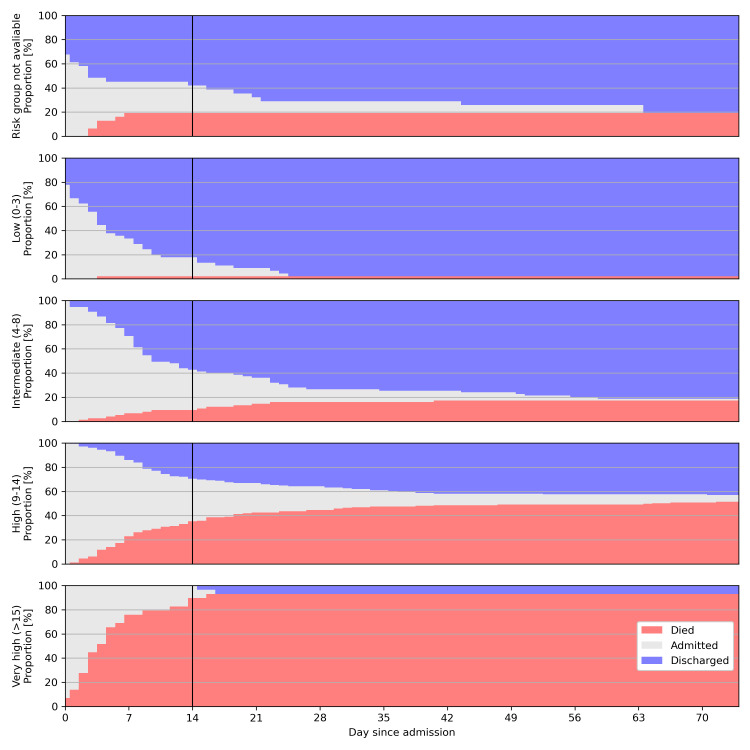
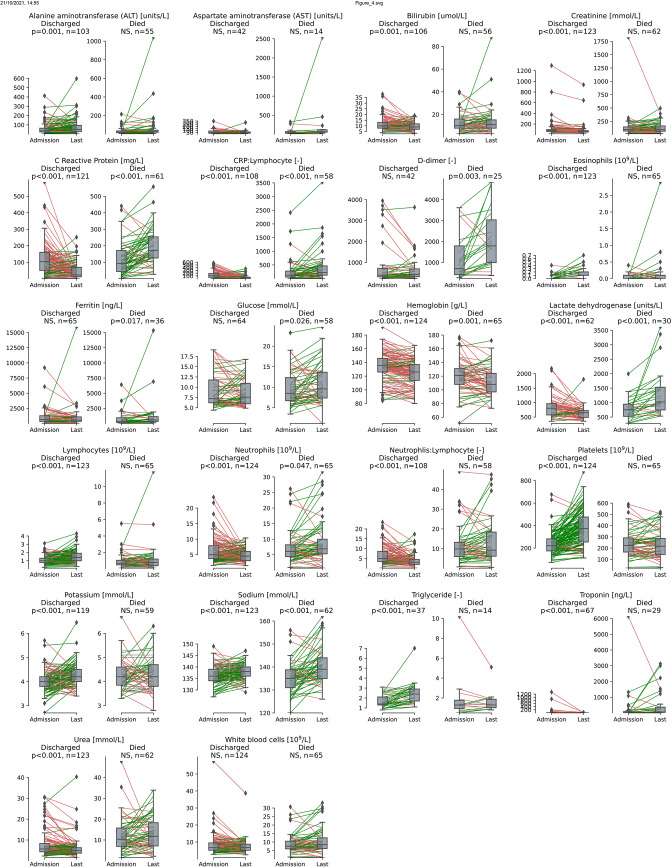
The majority of patients presented within 1 week of symptom onset. The lowest risk patients had low mortality (1/45, 2%), and most were discharged within 1 week after admission (30/45, 67%). The highest risk patients, as determined by the 4C mortality score predictor, had high mortality (27/29, 93%), with most dying within 1 week after admission (22/29, 76%). Consistent with previous reports, most patients presented with high levels of C reactive protein (CRP) (67% of patients >50 mg/L), D-dimer (98%>upper limit of normal (ULN)), ferritin (65%>ULN), lactate dehydrogenase (90%>ULN) and low lymphocyte counts (81%<lower limit of normal (LLN)). Increases in platelet counts and decreases in CRP, neutrophil:lymphocyte ratio (p<0.001), lactate dehydrogenase, neutrophil counts, urea and white cell counts (all p<0.01) were each associated with discharge.
Serial measurement of routine blood tests may be a useful prognostic tool for monitoring treatment response in hospitalised patients with COVID-19. Changes in other biochemical parameters often included in a 'COVID-19 bundle' did not show significant association with outcome, suggesting there may be limited clinical benefit of serial sampling. This may have direct clinical utility in the context of escalating healthcare costs of the pandemic.
COVID-19 是一种异质性疾病,许多报告描述了在发病时表现出的人口统计学、生化和临床特征的变化,这些变化影响着整体住院病死率。然而,关于 COVID-19 住院患者疾病进展过程中实验室预后变量的纵向变化的信息很少。
本回顾性观察性报告描述了在英格兰东南部的一家三级中心治疗的 COVID-19 患者从症状发作到住院、临床反应和出院/死亡的疾病进展情况。
在这项分析中,纳入了 2020 年 3 月至 9 月期间接受 SARS-CoV-2 治疗的 651 名患者。伦理批准由 HRA 特定审查委员会(REC 20/HRA/2986)获得,豁免了知情同意。
大多数患者在症状出现后 1 周内就诊。风险最低的患者死亡率较低(45 例中 1 例,2%),大多数在入院后 1 周内出院(45 例中 30 例,67%)。4C 死亡率评分预测器确定的风险最高的患者死亡率较高(29 例中 27 例,93%),大多数在入院后 1 周内死亡(29 例中 22 例,76%)。与先前的报告一致,大多数患者的 C 反应蛋白(CRP)水平较高(67%的患者>50mg/L),D-二聚体(98%>正常值上限(ULN))、铁蛋白(65%>ULN)、乳酸脱氢酶(90%>ULN)和淋巴细胞计数较低(81%<下限(LLN))。血小板计数增加,CRP、中性粒细胞:淋巴细胞比值(p<0.001)、乳酸脱氢酶、中性粒细胞计数、尿素和白细胞计数降低(均 p<0.01)均与出院相关。
连续测量常规血液检查可能是监测 COVID-19 住院患者治疗反应的有用预后工具。其他生化参数的变化,包括通常包含在“COVID-19 套餐”中的参数,与结局没有显著关联,这表明连续采样可能没有临床获益。这在大流行期间不断上升的医疗保健成本的背景下具有直接的临床应用价值。