Department of Psychology, University of Michigan, Ann Arbor.
Centre of Methods and Policy Application in the Social Sciences (COMPASS), University of Auckland, Auckland, New Zealand.
JAMA Psychiatry. 2022 Apr 1;79(4):333-340. doi: 10.1001/jamapsychiatry.2021.4377.
Mental disorders are an underappreciated category of modifiable risk factors for dementia. Developing an evidence base about the link between mental disorders and dementia risk requires studies that use large, representative samples, consider the full range of psychiatric conditions, ascertain mental disorders from early life, use long follow-ups, and distinguish between Alzheimer disease and related dementias.
To test whether mental disorders antedate dementia across 3 decades of observation.
DESIGN, SETTING, AND PARTICIPANTS: This population-based administrative register study of mental disorders and Alzheimer disease and related dementias included all individuals born in New Zealand between 1928 and 1967 who resided in the country for any time during the 30-year observation period between July 1988 and June 2018. Data were from the New Zealand Integrated Data Infrastructure, a collection of whole-of-population administrative data sources linked at the individual level. Data were analyzed from October 2020 to November 2021.
Diagnoses of mental disorders were ascertained from public-hospital records.
Diagnoses of dementia were ascertained from public-hospital records, mortality records, and pharmaceutical records.
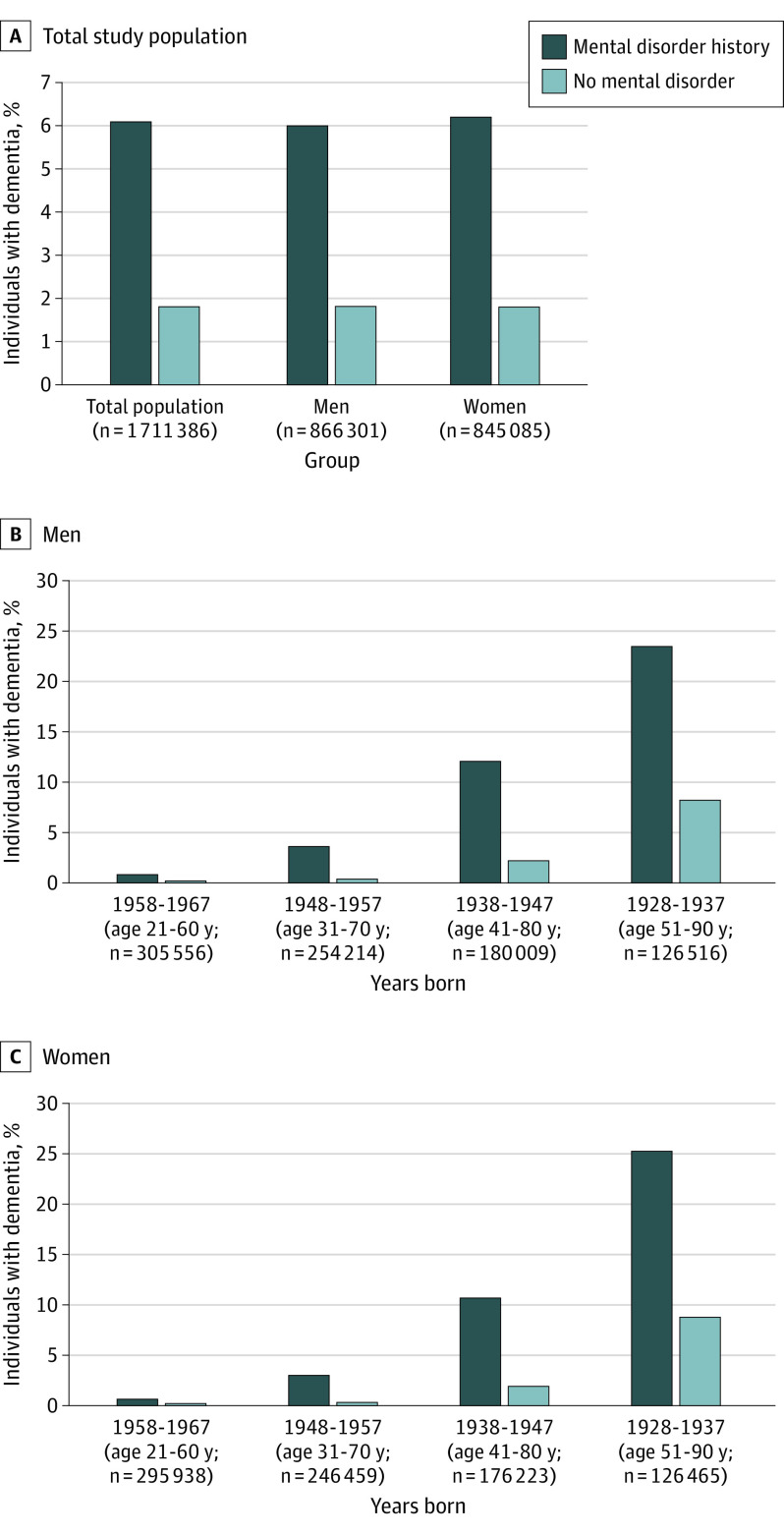
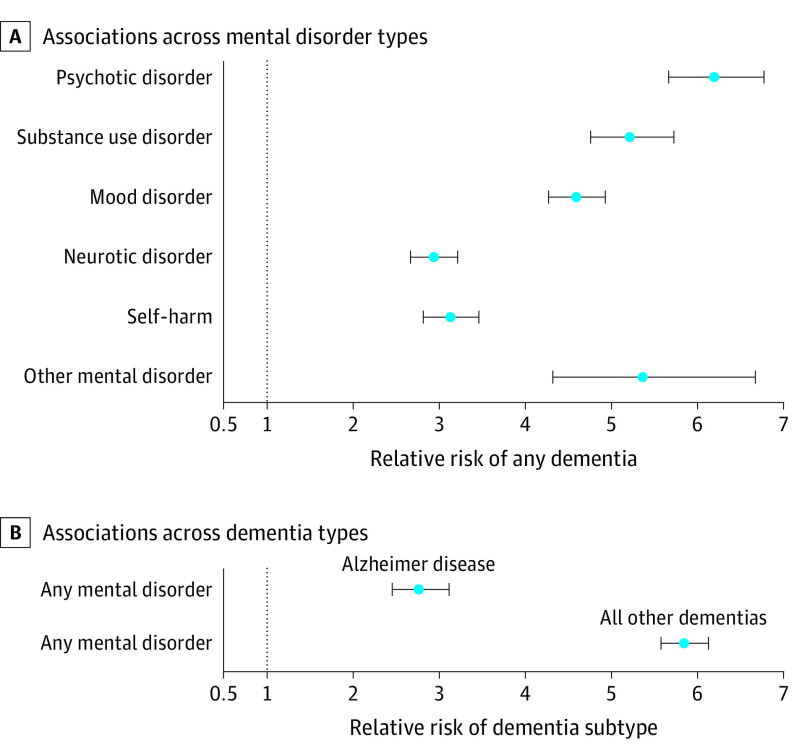
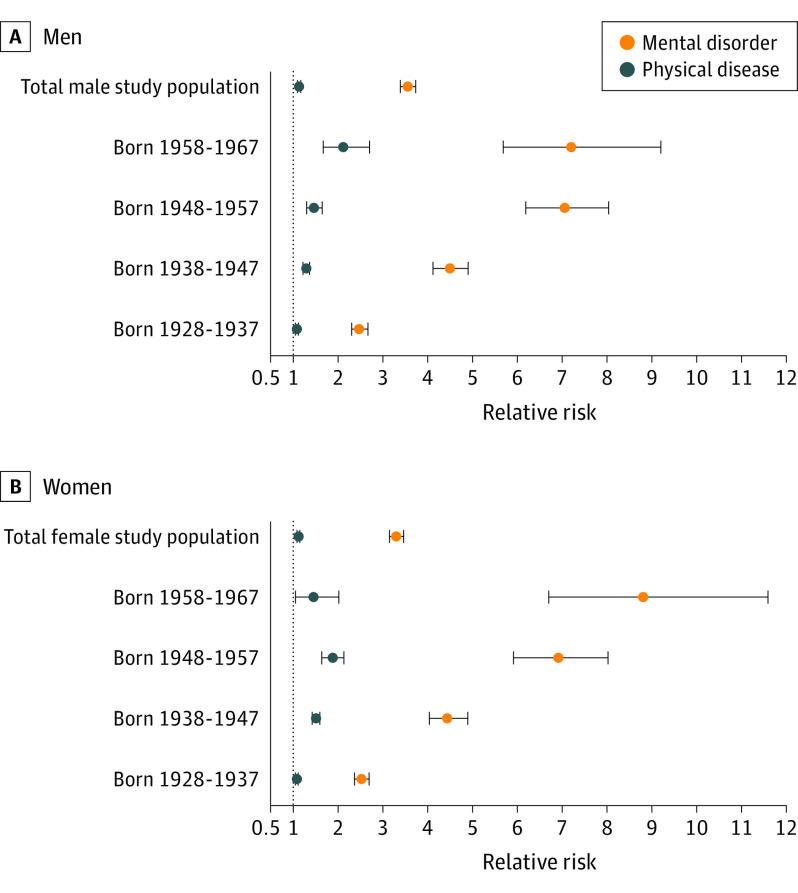
Of 1 711 386 included individuals, 866 301 (50.6%) were male, and individuals were aged 21 to 60 years at baseline. Relative to individuals without a mental disorder, those with a mental disorder were at increased risk of developing subsequent dementia (relative risk [RR], 4.24; 95% CI, 4.07-4.42; hazard ratio, 6.49; 95% CI, 6.25-6.73). Among individuals with dementia, those with a mental disorder developed dementia a mean of 5.60 years (95% CI, 5.31-5.90) earlier than those without a mental disorder. Associations held across sex and age and after accounting for preexisting chronic physical diseases and socioeconomic deprivation. Associations were present across different types of mental disorders and self-harm behavior (RRs ranged from 2.93 [95% CI, 2.66-3.21] for neurotic disorders to 6.20 [95% CI, 5.67-6.78] for psychotic disorders), and were evident for Alzheimer disease (RR, 2.76; 95% CI, 2.45-3.11) and all other dementias (RR, 5.85; 95% CI, 5.58-6.13).
In this study, mental disorders were associated with the onset of dementia in the population. Ameliorating mental disorders in early life might also ameliorate neurodegenerative conditions and extend quality of life in old age.
精神障碍是被低估的痴呆可改变的风险因素之一。为了建立精神障碍与痴呆风险之间的联系的证据基础,需要使用大型、有代表性的样本、考虑到全范围的精神疾病、从早期生活中确定精神障碍、使用长期随访,并区分阿尔茨海默病和相关痴呆症。
测试精神障碍是否在 30 年的观察中早于痴呆症。
设计、地点和参与者:这项基于人群的行政登记研究包括所有在新西兰出生于 1928 年至 1967 年之间的人,以及在 1988 年 7 月至 2018 年 6 月的 30 年观察期间在该国居住过的人。数据来自新西兰综合数据基础设施,这是一个收集了整个人口行政数据来源并在个人层面上进行链接的集合。数据从 2020 年 10 月至 2021 年 11 月进行分析。
精神障碍的诊断是从公立医院记录中确定的。
痴呆症的诊断是从公立医院记录、死亡率记录和药物记录中确定的。
在纳入的 1711386 人中,866301 人(50.6%)为男性,基线时年龄在 21 至 60 岁之间。与没有精神障碍的人相比,有精神障碍的人患后续痴呆症的风险更高(相对风险 [RR],4.24;95%CI,4.07-4.42;危险比,6.49;95%CI,6.25-6.73)。在患有痴呆症的人中,有精神障碍的人比没有精神障碍的人早平均 5.60 年(95%CI,5.31-5.90)发展为痴呆症。关联在性别和年龄之间都存在,并且考虑到预先存在的慢性躯体疾病和社会经济剥夺因素后仍然存在。关联存在于不同类型的精神障碍和自残行为(RR 范围从神经症障碍的 2.93 [95%CI,2.66-3.21] 到精神病障碍的 6.20 [95%CI,5.67-6.78]),以及阿尔茨海默病(RR,2.76;95%CI,2.45-3.11)和所有其他痴呆症(RR,5.85;95%CI,5.58-6.13)。
在这项研究中,精神障碍与人群中痴呆症的发生有关。在生命早期改善精神障碍也可能改善神经退行性疾病,并延长老年时的生活质量。