Awasthi Puspraj, Kumar Vijay, Naganur Sanjeev, Nallasamy Karthi, Angurana Suresh Kumar, Bansal Arun, Manoj Rohit Kumar, Jayashree Muralidharan
Division of Pediatric Critical Care, Department of Pediatrics, Advanced Pediatrics Centre, Chandigarh, India.
Department of Cardiology, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India.
Am J Trop Med Hyg. 2022 Feb 16;106(4):1108-1112. doi: 10.4269/ajtmh.21-0801. Print 2022 Apr 6.
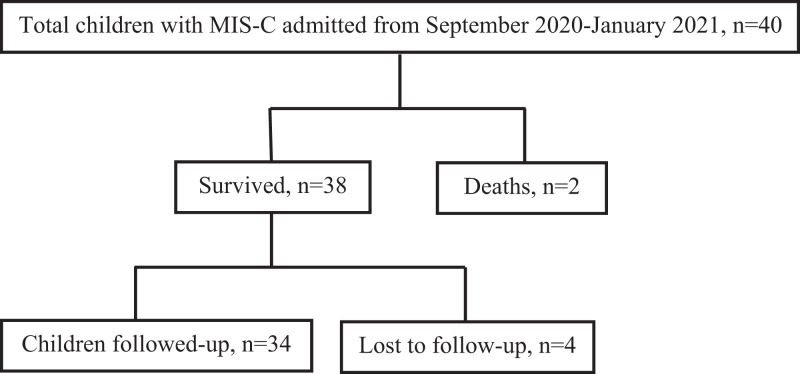
Multisystem inflammatory syndrome in children (MIC-S) is a hyperinflammatory manifestation of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection. Information on the long-term outcome of MIS-C is limited. This study was conducted to describe the long-term outcome of MIS-C from a tertiary care center in North India. Children admitted with MIS-C from September 2020 to January 2021 were followed up after discharge until June 2021. The details during the acute phase (clinical features, investigations, treatment, and outcome) and follow-up (symptoms, echocardiographic findings, ongoing treatment, and outcome) were collected retrospectively. During the acute phase, 40 children presented at median (interquartile range [IQR]) age of 7 (5-10) years with fever, mucocutaneous, gastrointestinal, and respiratory symptoms. The majority (66.7%) of the children had positive SARS-CoV-2 serology and elevated inflammatory markers (C-reactive protein, procalcitonin, ferritin, D-dimer, and fibrinogen), lymphopenia, and thrombocytopenia. Eighty percent had shock, 72.5% had myocardial dysfunction (left ventricular ejection fraction <55%), and 22.5% had coronary artery dilatation or aneurysm. Treatment included pediatric intensive care unit admission (85%), intravenous immunoglobulin (100%), steroids (85%), aspirin (80%), vasoactive drugs (72.5%), and invasive mechanical ventilation (22.5%). Two (5%) children died because of refractory shock. Thirty-four children were followed up with until a median (IQR) of 5 (3-6) months. During the follow-up, a majority were asymptomatic, myocardial function returned to normal in all, and only one had coronary artery aneurysm. Prednisolone and aspirin were given for a median (IQR) of 3 (2-4) weeks and 4 (4-6) weeks after discharge, respectively. There was one readmission and no death during the follow-up. To conclude, the long-term outcome of MIS-C is generally favorable with resolution of cardiovascular manifestations (myocardial dysfunction and coronary artery changes) in the majority of children during follow-up.
儿童多系统炎症综合征(MIS-C)是严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染的一种过度炎症表现。关于MIS-C长期预后的信息有限。本研究旨在描述印度北部一家三级医疗中心MIS-C的长期预后情况。对2020年9月至2021年1月因MIS-C入院的儿童在出院后进行随访,直至2021年6月。回顾性收集急性期(临床特征、检查、治疗及预后)和随访期(症状、超声心动图检查结果、持续治疗及预后)的详细信息。急性期有40名儿童,中位(四分位间距[IQR])年龄为7(5 - 10)岁,出现发热、皮肤黏膜、胃肠道及呼吸道症状。大多数(66.7%)儿童SARS-CoV-2血清学检测呈阳性,炎症标志物(C反应蛋白、降钙素原、铁蛋白、D - 二聚体和纤维蛋白原)升高,淋巴细胞减少,血小板减少。80%的儿童出现休克,72.5%有心肌功能障碍(左心室射血分数<55%),22.5%有冠状动脉扩张或动脉瘤。治疗包括入住儿科重症监护病房(85%)、静脉注射免疫球蛋白(100%)、使用类固醇(85%)、阿司匹林(80%)、血管活性药物(72.5%)及有创机械通气(22.5%)。两名(5%)儿童因难治性休克死亡。34名儿童接受随访,中位(IQR)随访时间为5(3 - 6)个月。随访期间,大多数儿童无症状,所有儿童心肌功能恢复正常,仅1名儿童有冠状动脉瘤。出院后分别给予泼尼松龙和阿司匹林的中位(IQR)时间为3(2 - 4)周和4(4 - 6)周。随访期间有1名儿童再次入院,无死亡病例。总之,MIS-C的长期预后总体良好,大多数儿童在随访期间心血管表现(心肌功能障碍和冠状动脉改变)得到缓解。