Shobhavat Lakshmi, Solomon Rekha, Rao Sudha, Bhagat Isha, Prabhu Sanjay, Prabhu Shakuntala, Chandrakar Manoj, Bodhanwala Minnie
Department of PICU, Bai Jerbai Wadia Hospital for Children, Mumbai, Maharashtra, India.
Department of Pediatrics, Bai Jerbai Wadia Hospital for Children, Mumbai, Maharashtra, India.
Indian J Crit Care Med. 2020 Nov;24(11):1089-1094. doi: 10.5005/jp-journals-10071-23658.
Multisystem inflammatory syndrome (MIS) associated with severe acute respiratory syndrome coronavirus (SARS-CoV-2) (MIS-C) in children is being increasingly reported across the world.
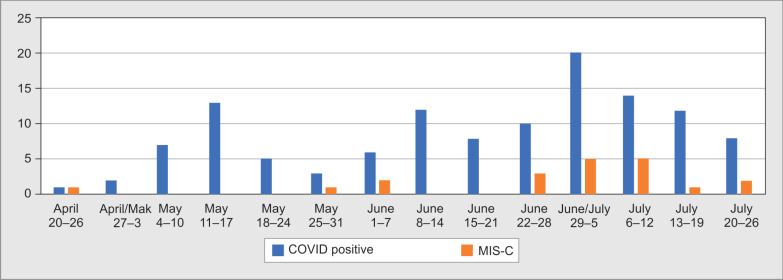
Children fulfilling the World Health Organization criteria of MIS-C needing pediatric intensive care unit between April 15 and July 26, 2020 were studied.
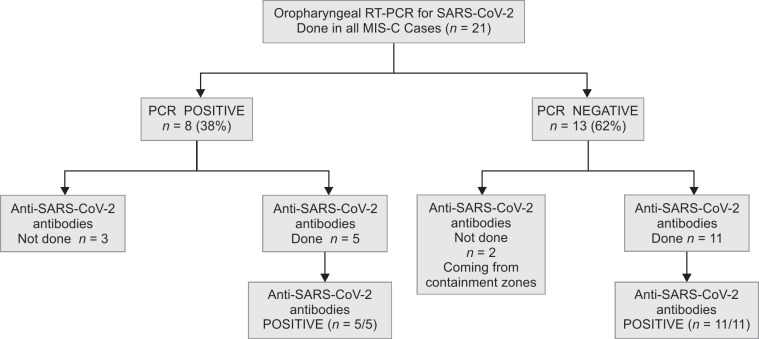
There were 21 patients with median age of 7 years [interquartile range (IQR) 1.9-12.1], of which 11 were females. SARS-CoV-2 real-time polymerase chain reaction positive in 8/21 and/or antibody positive 16/21. Fever was present in all patients, and gastrointestinal symptoms being second most frequent (16/21). One child had aplastic anemia, while the rest had no comorbidities. Nearly all presented with shock ( = 20/21) and 90% needed vasoactive drugs with a median Vasoactive Inotropic Score of 40 (IQR 20-95). Thirteen children needed ventilatory support and one needed peritoneal dialysis. Nine children had left ventricular dysfunction and five had dilatation of coronaries on echocardiography. Inflammatory markers C-reactive protein [98 mg/dL (IQR 89-119)], serum ferritin [710 mg/dL (IQR 422-1,609)], and serum interleukin-6 levels [215 ng/L (IQR 43-527)] were uniformly elevated. Eighteen children received pulse methyl-prednisolone, eleven intravenous immunoglobulins, and four tocilizumab. Eighteen children (86%) were discharged home while three died.
In our cohort, MIS-C was seen in previously healthy children with fever, gastrointestinal symptoms, and shock. Early and aggressive management of shock and immune modulation with methyl-prednisolone and intravenous immunoglobulin were used.
Shobhavat L, Solomon R, Rao S, Bhagat I, Prabhu S, Prabhu S, Multisystem Inflammatory Syndrome in Children: Clinical Features and Management-Intensive Care Experience from a Pediatric Public Hospital in Western India. Indian J Crit Care Med 2020;24(11):1089-1094.
全球范围内,儿童多系统炎症综合征(MIS)与严重急性呼吸综合征冠状病毒2(SARS-CoV-2)相关(MIS-C)的报道日益增多。
对2020年4月15日至7月26日期间符合世界卫生组织MIS-C标准且需要入住儿科重症监护病房的儿童进行研究。
共21例患者,中位年龄7岁[四分位间距(IQR)1.9 - 12.1],其中11例为女性。21例中8例SARS-CoV-2实时聚合酶链反应呈阳性和/或16例抗体呈阳性。所有患者均有发热,胃肠道症状是第二常见症状(21例中的16例)。1例儿童患有再生障碍性贫血,其余无合并症。几乎所有患者均出现休克(21例中的20例),90%需要血管活性药物,血管活性药物评分中位数为40(IQR 20 - 95)。13例儿童需要通气支持,1例需要腹膜透析。9例儿童有左心室功能障碍,5例超声心动图显示冠状动脉扩张。炎症标志物C反应蛋白[98mg/dL(IQR 89 - 119)]、血清铁蛋白[710mg/dL(IQR 422 - 1609)]和血清白细胞介素-6水平[215ng/L(IQR 43 - 527)]均普遍升高。18例儿童接受了甲泼尼龙冲击治疗,11例接受了静脉注射免疫球蛋白治疗,4例接受了托珠单抗治疗。18例儿童(86%)出院回家,3例死亡。
在我们的队列中,MIS-C见于既往健康的儿童,表现为发热、胃肠道症状和休克。采用了早期积极的休克治疗以及甲泼尼龙和静脉注射免疫球蛋白进行免疫调节。
Shobhavat L, Solomon R, Rao S, Bhagat I, Prabhu S, Prabhu S, 儿童多系统炎症综合征:临床特征与管理——印度西部一家儿科公立医院的重症监护经验。《印度危重症医学杂志》2020;24(11):1089 - 1094。