Szoka Nova, Kahn Mathew
Department of Surgery, West Virginia University, 1 Medical Center Dr., Morgantown, WV 26505, USA.
West Virginia University School of Medicine, USA.
Case Rep Surg. 2022 Feb 7;2022:5459774. doi: 10.1155/2022/5459774. eCollection 2022.
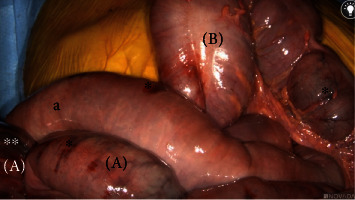
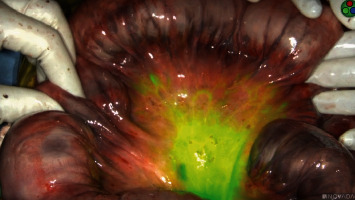
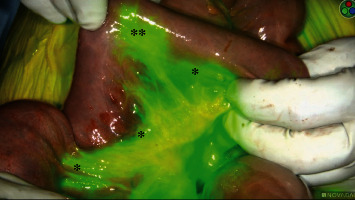
Mesenteric ischemia (MI) is a condition characterized by compromised intestinal perfusion, leading to varied patterns of bowel hypoxia that requires prompt diagnosis and surgical intervention. Here, we report a case in which indocyanine green (ICG) was utilized to evaluate intestinal blood flow in a patient with acute-on-chronic MI. A 65-year-old underweight female presented with abdominal pain out of proportion to exam and was found to have diffuse aortic atherosclerotic disease with chronic occlusion of both superior and inferior mesenteric arteries with distal reconstitution. After multidisciplinary evaluation, elective treatment with vascular surgery was planned; however, on day three of her hospitalization, the patient's abdominal pain acutely worsened. She was taken to the OR for exploratory laparotomy. Under white light, the small bowel from the ligament of Treitz (LOT) to the terminal ileum and the large bowel from the cecum to the splenic flexure appeared ischemic with patchy areas of necrosis. Fluorescence angiography was then performed; injection of indocyanine green (ICG) dye and imaging with the SPY-PHI near-infrared camera system demonstrated appropriate blood flow into the bowel mesentery, with complete absence of flow into the bowel mucosal surface from the LOT to the splenic flexure, confirming irreversible bowel necrosis. Introduction of ICG intraoperatively decreased the uncertainty associated with white light assessment of bowel viability, leading to a definitive intraoperative diagnosis and clear plan of care. The use of fluorescence guidance to diagnose fulminant small and large bowel necrosis prevented the surgical team from having to perform multiple takebacks to the operating room in the setting of a nonsurvivable injury. Had the surgical team relied on the white light appearance of the bowel, they would not have been able to diagnose the true extent of bowel demise. The patient was placed on comfort care for this devastating nonsurvivable injury.
肠系膜缺血(MI)是一种以肠道灌注受损为特征的病症,会导致多种形式的肠缺氧,需要及时诊断和手术干预。在此,我们报告一例使用吲哚菁绿(ICG)评估一名慢性肠系膜缺血急性发作患者肠道血流的病例。一名65岁体重不足的女性因腹痛与检查结果不符前来就诊,经检查发现患有弥漫性主动脉粥样硬化疾病,肠系膜上动脉和肠系膜下动脉均慢性闭塞且有远端血管重建。经过多学科评估后,计划进行血管外科择期治疗;然而,在她住院的第三天,患者腹痛急剧加重。她被送往手术室进行剖腹探查术。在白光下,从屈氏韧带(LOT)至回肠末端的小肠以及从盲肠至脾曲的大肠均呈现缺血状态,伴有散在的坏死区域。随后进行了荧光血管造影;注射吲哚菁绿(ICG)染料并使用SPY-PHI近红外摄像系统成像显示,肠道系膜有适当的血流进入,但从LOT至脾曲的肠道黏膜表面完全没有血流,证实存在不可逆的肠坏死。术中引入ICG降低了与白光评估肠活力相关的不确定性,从而得出明确的术中诊断和清晰的护理计划。使用荧光引导诊断暴发性小肠和大肠坏死避免了手术团队在面对不可存活损伤时多次返回手术室。如果手术团队仅依靠肠道的白光外观,他们将无法诊断出肠道坏死的真实程度。鉴于这种毁灭性的不可存活损伤,该患者接受了舒适护理。