Center for Sarcoma and Bone Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts.
Department of Biostatistics, University of Colorado Anschutz Medical Campus, Aurora, Colorado.
Clin Cancer Res. 2022 Sep 15;28(18):4092-4104. doi: 10.1158/1078-0432.CCR-21-4504.
Determine whether specific CTNNB1 or APC mutations in patients with desmoid tumor were associated with differences in clinical responses to systemic treatments.
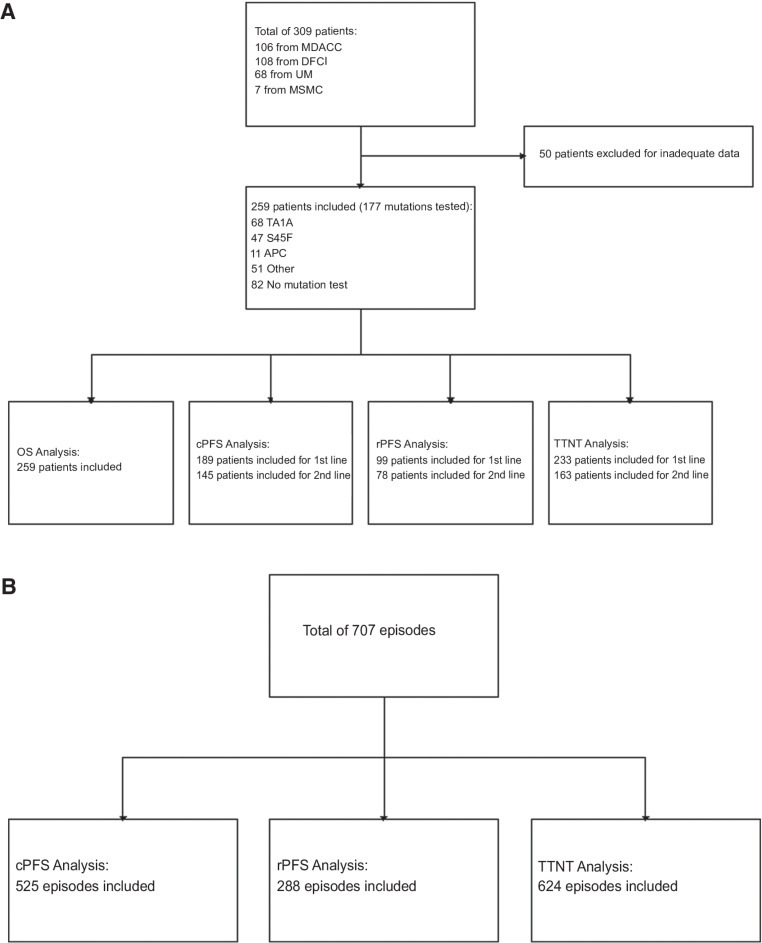
We established a multi-institutional dataset of previously treated patients with desmoid tumor across four U.S. sarcoma centers, including demographic and clinicopathologic characteristics, treatment regimens, and clinical and radiographic responses. CTNNB1 or APC mutation status was determined from prior pathology records, or archival tissue was requested and analyzed by Sanger sequencing and/or next-generation sequencing. Evaluable patients with mutation results were analyzed to determine clinical progression-free survival (cPFS), RECIST 1.1 PFS (rPFS), time to next treatment (TTNT), and overall survival (OS). Kaplan-Meier analysis and Cox proportional hazards regression were performed to identify differences in cPFS, rPFS, TTNT, and OS by mutation subtype, desmoid tumor location, and treatment regimen.
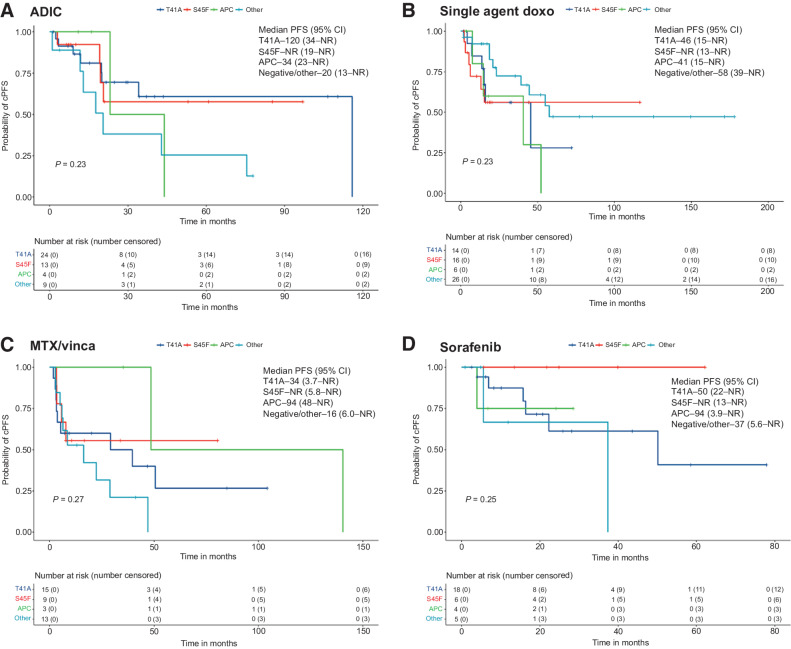
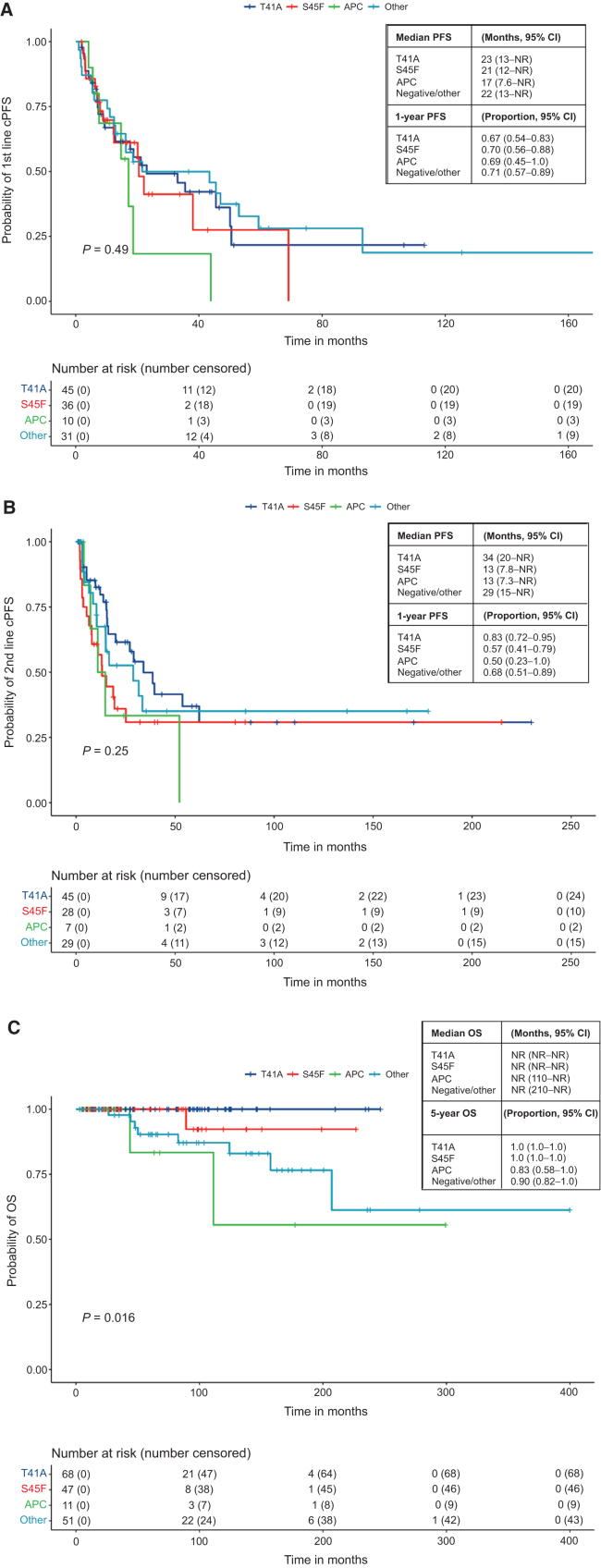
A total of 259 evaluable patients were analyzed for at least one of the survival outcomes, with 177 patients having mutation data. First- and second-line cPFS, rPFS, and TTNT were not significantly affected by mutation subtype; however, APC-mutant desmoid tumors demonstrated nonstatistically significant inferior outcomes. Extremity/trunk desmoid tumor location and treatment with doxorubicin-based, methotrexate/vinca alkaloids and sorafenib regimens were associated with better clinical outcomes compared with surgery or "other" therapies, including estrogen-receptor blockade and imatinib. OS was significantly worse with APC or CTNNB1 negative/other mutations.
Mutation subtype did not affect responses to specific systemic therapies. APC mutations and nonextremity desmoid tumor locations remain prognostic for worse outcomes, and earlier initiation of systemic therapy for these higher-risk desmoid tumors should be prospectively evaluated. See related commentary by Greene and Van Tine, p. 3911.
确定患有硬纤维瘤的患者中 CTNNB1 或 APC 突变是否与全身治疗的临床反应差异相关。
我们建立了一个由四个美国肉瘤中心的先前治疗过的硬纤维瘤患者组成的多机构数据集,包括人口统计学和临床病理学特征、治疗方案以及临床和放射学反应。CTNNB1 或 APC 突变状态是从先前的病理记录中确定的,或者请求并通过 Sanger 测序和/或下一代测序分析存档组织。分析有突变结果的可评估患者,以确定临床无进展生存期 (cPFS)、RECIST 1.1 PFS (rPFS)、下一次治疗时间 (TTNT) 和总生存期 (OS)。进行 Kaplan-Meier 分析和 Cox 比例风险回归,以确定突变亚型、硬纤维瘤位置和治疗方案对 cPFS、rPFS、TTNT 和 OS 的差异。
共分析了 259 名至少有一项生存结果的可评估患者,其中 177 名患者有突变数据。首次和第二次 cPFS、rPFS 和 TTNT 未受突变亚型显著影响;然而,APC 突变的硬纤维瘤表现出非统计学上较差的结果。肢体/躯干硬纤维瘤位置和使用多柔比星、甲氨蝶呤/长春花生物碱和索拉非尼方案治疗与手术或“其他”疗法相比,包括雌激素受体阻断和伊马替尼,具有更好的临床结果。APC 或 CTNNB1 阴性/其他突变的 OS 明显更差。
突变亚型不会影响特定全身治疗的反应。APC 突变和非肢体硬纤维瘤位置仍然是预后较差的标志,对于这些高风险的硬纤维瘤,应前瞻性评估更早开始全身治疗。见 Greene 和 Van Tine 的相关评论,第 3911 页。