Qutub Mohammed, Aldabbagh Yasser, Mehdawi Fahtima, Alraddadi Abdullah, Alhomsy Mohanna, Alnahdi Abdulaziz, Fakeeh Majed, Maghrabi Abdullah, Alwagdani Meshari, Bahabri Nezar
Department of Pathology and Laboratory Medicine, King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia.
Adult Infectious Diseases division, Department of Medicine, King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia.
Clin Infect Pract. 2022 Jan;13:100140. doi: 10.1016/j.clinpr.2022.100140. Epub 2022 Feb 16.
The duration of viable viral shedding is important to be defined in regards of viral transmission in SARS-CoV-2 infection with the backdrop of the current worldwide effort for revising isolation polices and establishing the duration of infectiousness.
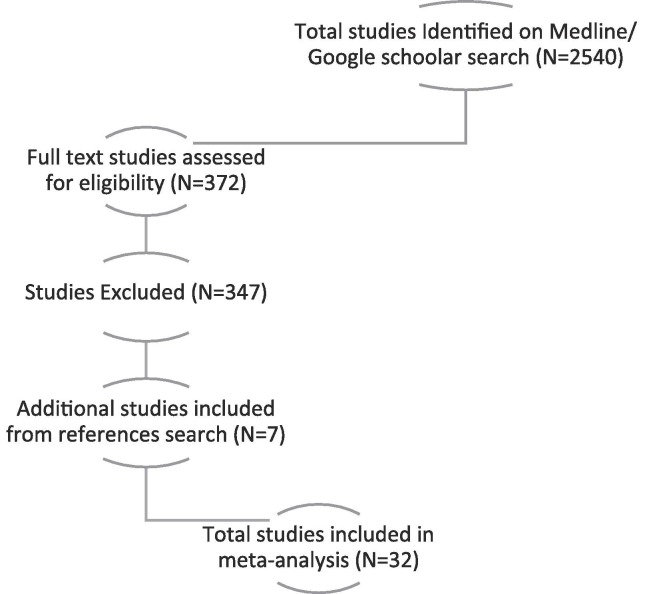
In this review we searched databases including Medline and google scholar for research articles published between January 2020 and January 2022. We included case reports, case series, cross sectional, cohort, and randomized control trials that reported the duration of shedding of viable SARS-CoV-2 virus. After evaluating the criteria for inclusion, 32 articles (2721 patients) were included.
This review showed that the median for the last day of successful viral isolation was 11 (8.5-14.5 95% CI) , 20 (9.0-57.5 95 %CI), 20 (9.0-103 95 %CI) for the general population, critical patients and immunocompromised individuals, respectively, with significant association between prolonged viral shedding, disease severity (P-Value 0.024) and immunosuppressive status (P-Value 0.023).The corresponding higher cutoff of CTv to culturable virus ranged between 26.25 and 34.00 (95% confidence interval) with median of 30.5, and higher values were observed when critical (25.0-37.37 95 %CI) and immunocompromised patients (20.0-37.82 95 %CI) have been excluded, this deviation did not represent a statistical significance (P-Value 0.997 and 0.888) respectively.
Our review highlights that repeating SARS-CoV-2 viral RNA test solely in recovering patients has no importance in determining infectivity and emphasizes the individualization of de-isolation decisions based on the host factors and a combined symptom and testing-based approaches with the later benefiting most of correlation with recently introduced rapid antigen test. Our finding in the review also opposes the most recent CDC Guidance on shortening isolation duration in term of the last days of viable transmissible virus, therefore caution should be considered when revising such protocols.
在当前全球努力修订隔离政策并确定传染性持续时间的背景下,明确严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染中病毒存活脱落的持续时间对于病毒传播至关重要。
在本综述中,我们检索了包括Medline和谷歌学术在内的数据库,以查找2020年1月至2022年1月发表的研究文章。我们纳入了报告SARS-CoV-2活病毒脱落持续时间的病例报告、病例系列、横断面研究、队列研究和随机对照试验。在评估纳入标准后,纳入了32篇文章(2721名患者)。
本综述表明,成功病毒分离的最后一天的中位数,普通人群为11天(8.5 - 14.5,95%置信区间),重症患者为20天(9.0 - 57.5,95%置信区间),免疫功能低下个体为20天(9.0 - 103,95%置信区间),病毒脱落延长与疾病严重程度(P值0.024)和免疫抑制状态(P值0.023)之间存在显著关联。可培养病毒的相应较高CTv临界值在26.25至34.00之间(95%置信区间),中位数为30.5,当排除重症患者(25.0 - 37.37,95%置信区间)和免疫功能低下患者(20.0 - 37.82,95%置信区间)时观察到更高的值,这种偏差分别不具有统计学意义(P值0.997和0.888)。
我们的综述强调,仅对康复患者重复进行SARS-CoV-2病毒RNA检测对确定传染性并无重要意义,并强调基于宿主因素以及症状与检测相结合的方法来个体化解除隔离决策,后者因与最近推出的快速抗原检测相关性最强而受益最大。我们在综述中的发现也与美国疾病控制与预防中心(CDC)关于缩短可行传播病毒最后几天隔离时间的最新指南相悖,因此在修订此类方案时应谨慎考虑。