Institute of Infection and Global Health, University of Liverpool, Liverpool, UK; Institute of Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town, South Africa; Liverpool School of Tropical Medicine, Liverpool, UK.
Liverpool School of Tropical Medicine, Liverpool, UK; Malawi-Liverpool-Wellcome Clinical Research Programme, Queen Elizabeth Central Hospital, College of Medicine, Blantyre, Malawi.
Lancet Infect Dis. 2020 Jun;20(6):742-752. doi: 10.1016/S1473-3099(19)30695-4. Epub 2020 Mar 13.
The clinical and epidemiological significance of HIV-associated Mycobacterium tuberculosis bloodstream infection (BSI) is incompletely understood. We hypothesised that M tuberculosis BSI prevalence has been underestimated, that it independently predicts death, and that sputum Xpert MTB/RIF has suboptimal diagnostic yield for M tuberculosis BSI.
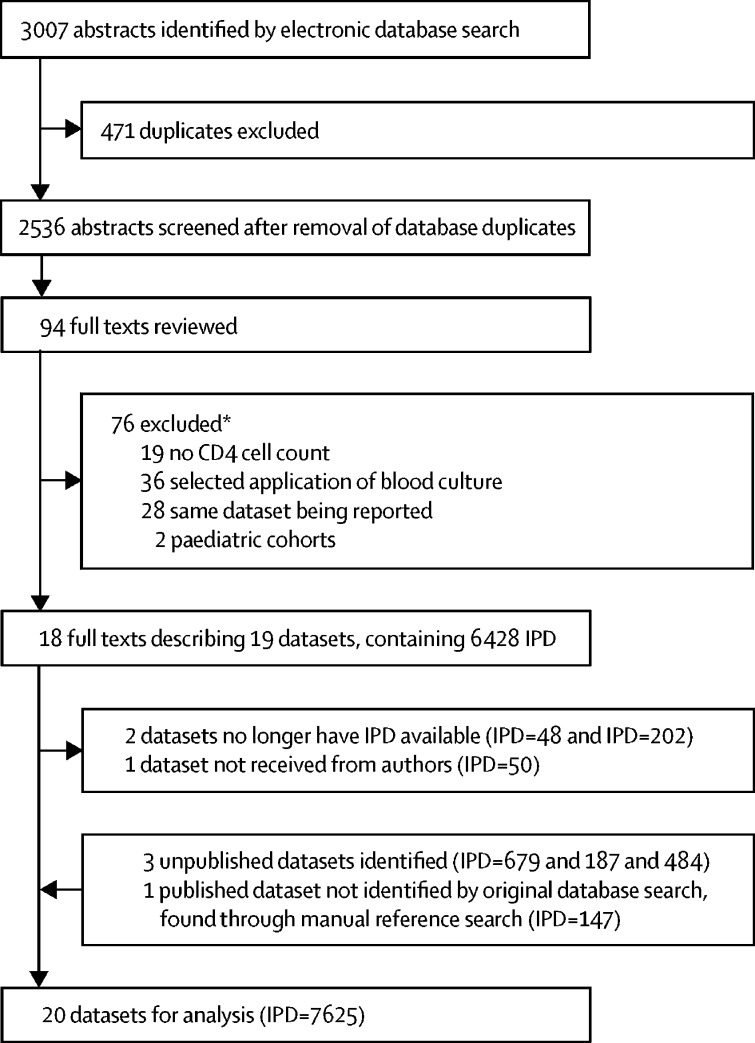
We did a systematic review and individual patient data (IPD) meta-analysis of studies performing routine mycobacterial blood culture in a prospectively defined patient population of people with HIV aged 13 years or older. Studies were identified through searching PubMed and Scopus up to Nov 10, 2018, without language or date restrictions and through manual review of reference lists. Risk of bias in the included studies was assessed with an adapted QUADAS-2 framework. IPD were requested for all identified studies and subject to harmonised inclusion criteria: age 13 years or older, HIV positivity, available CD4 cell count, a valid mycobacterial blood culture result (excluding patients with missing data from lost or contaminated blood cultures), and meeting WHO definitions for suspected tuberculosis (presence of screening symptom). Predicted probabilities of M tuberculosis BSI from mixed-effects modelling were used to estimate prevalence. Estimates of diagnostic yield of sputum testing with Xpert (or culture if Xpert was unavailable) and of urine lipoarabinomannan (LAM) testing for M tuberculosis BSI were obtained by two-level random-effect meta-analysis. Estimates of mortality associated with M tuberculosis BSI were obtained by mixed-effect Cox proportional-hazard modelling and of effect of treatment delay on mortality by propensity-score analysis. This study is registered with PROSPERO, number 42016050022.
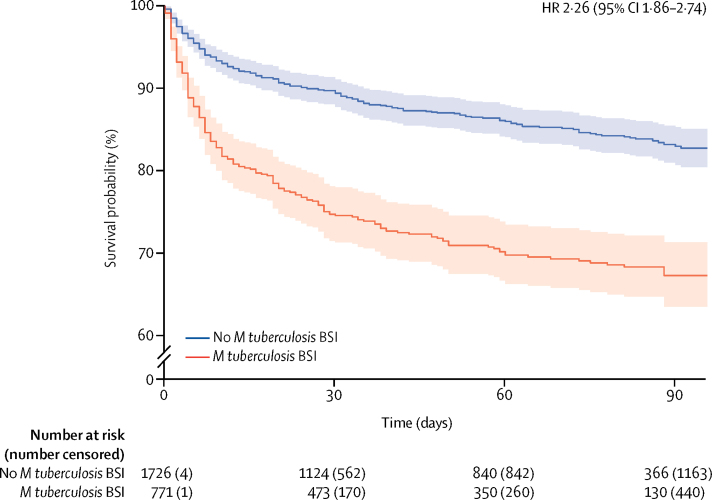
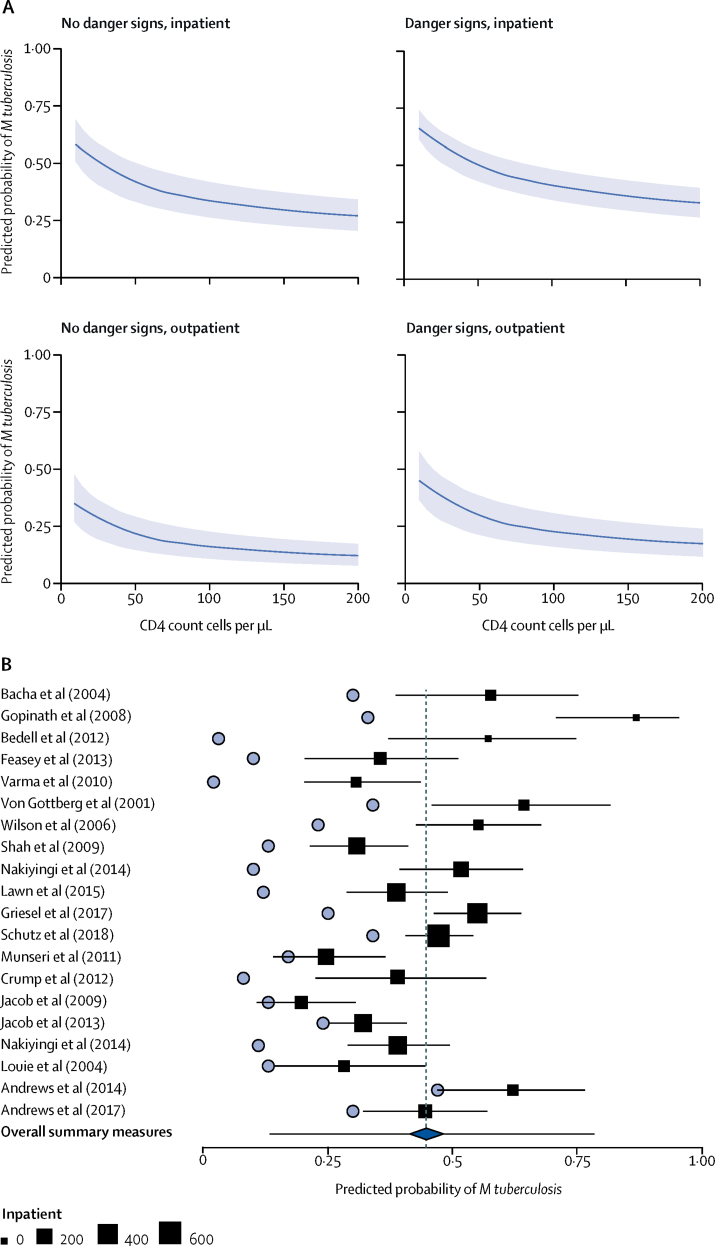
We identified 23 datasets for inclusion (20 published and three unpublished at time of search) and obtained IPD from 20, representing 96·2% of eligible IPD. Risk of bias for the included studies was assessed to be generally low except for on the patient selection domain, which was moderate in most studies. 5751 patients met harmonised IPD-level inclusion criteria. Technical factors such as number of blood cultures done, timing of blood cultures relative to blood sampling, and patient factors such as inpatient setting and CD4 cell count, explained significant heterogeneity between primary studies. The predicted probability of M tuberculosis BSI in hospital inpatients with HIV-associated tuberculosis, WHO danger signs, and a CD4 count of 76 cells per μL (the median for the cohort) was 45% (95% CI 38-52). The diagnostic yield of sputum in patients with M tuberculosis BSI was 77% (95% CI 63-87), increasing to 89% (80-94) when combined with urine LAM testing. Presence of M tuberculosis BSI compared with its absence in patients with HIV-associated tuberculosis increased risk of death before 30 days (adjusted hazard ratio 2·48, 95% CI 2·05-3·08) but not after 30 days (1·25, 0·84-2·49). In a propensity-score matched cohort of participants with HIV-associated tuberculosis (n=630), mortality increased in patients with M tuberculosis BSI who had a delay in anti-tuberculosis treatment of longer than 4 days compared with those who had no delay (odds ratio 3·15, 95% CI 1·16-8·84).
In critically ill adults with HIV-tuberculosis, M tuberculosis BSI is a frequent manifestation of tuberculosis and predicts mortality within 30 days. Improved diagnostic yield in patients with M tuberculosis BSI could be achieved through combined use of sputum Xpert and urine LAM. Anti-tuberculosis treatment delay might increase the risk of mortality in these patients.
This study was supported by Wellcome fellowships 109105Z/15/A and 105165/Z/14/A.
HIV 相关分枝杆菌血流感染(BSI)的临床和流行病学意义尚不完全清楚。我们假设 M 结核分枝杆菌 BSI 的患病率被低估了,它独立预测死亡,并且痰 Xpert MTB/RIF 对 M 结核分枝杆菌 BSI 的诊断效果不佳。
我们对前瞻性定义的 HIV 成人患者人群中进行常规分枝杆菌血液培养的研究进行了系统评价和个体患者数据(IPD)荟萃分析。通过在 2018 年 11 月 10 日之前搜索 PubMed 和 Scopus 来确定研究,无语言或日期限制,并通过手动审查参考文献来确定。使用适应性 QUADAS-2 框架评估纳入研究的偏倚风险。请求所有确定的研究提供 IPD,并进行协调纳入标准:年龄 13 岁或以上,HIV 阳性,可用 CD4 细胞计数,有效的分枝杆菌血液培养结果(排除因丢失或污染血液培养而导致数据缺失的患者),并符合世卫组织对疑似结核病的定义(存在筛查症状)。从混合效应建模中预测 M 结核分枝杆菌 BSI 的概率用于估计患病率。通过两级随机效应荟萃分析获得痰检测(如果 Xpert 不可用,则进行培养)和尿液脂阿拉伯甘露聚糖(LAM)检测对 M 结核分枝杆菌 BSI 的诊断效果的估计。通过混合效应 Cox 比例风险模型获得与 M 结核分枝杆菌 BSI 相关的死亡率的估计,以及通过倾向评分分析获得治疗延迟对死亡率的影响。本研究在 PROSPERO 注册,编号为 42016050022。
我们确定了 23 个数据集(20 个已发表,3 个在搜索时未发表),并从 20 个中获得了 IPD,代表了 96.2%的合格 IPD。纳入研究的偏倚风险通常较低,但在患者选择方面中等,大多数研究都存在。5751 名患者符合 IPD 级别的纳入标准。技术因素,如血液培养的数量,血液培养相对于血液采样的时间,以及患者因素,如住院环境和 CD4 细胞计数,解释了主要研究之间的显著异质性。HIV 相关结核病、世卫组织危险信号和 CD4 计数为 76 个细胞/μL(队列中位数)的住院患者中 M 结核分枝杆菌 BSI 的预测概率为 45%(95%CI 38-52)。在 M 结核分枝杆菌 BSI 患者中,痰的诊断效果为 77%(95%CI 63-87),当与尿液 LAM 检测联合使用时,增加到 89%(80-94)。与 HIV 相关结核病患者相比,M 结核分枝杆菌 BSI 的存在增加了 30 天内死亡的风险(调整后的危险比 2.48,95%CI 2.05-3.08),但在 30 天之后没有增加(1.25,0.84-2.49)。在一组 630 名 HIV 相关结核病患者的倾向评分匹配队列中,与没有延迟的患者相比,抗结核治疗延迟超过 4 天的 M 结核分枝杆菌 BSI 患者的死亡率增加(比值比 3.15,95%CI 1.16-8.84)。
在患有 HIV-结核病的重症成年人中,M 结核分枝杆菌 BSI 是结核病的常见表现,并预测 30 天内的死亡率。通过联合使用痰 Xpert 和尿液 LAM,可提高 M 结核分枝杆菌 BSI 患者的诊断效果。抗结核治疗延迟可能会增加这些患者的死亡率。
本研究得到了惠康基金会 109105Z/15/A 和 105165/Z/14/A 的资助。