Centre for Health Systems and Safety Research, Australian Institute of Health Innovation, Macquarie University, Australia.
Clinical Excellence Commission, Sydney, Australia.
J Med Internet Res. 2022 Feb 23;24(2):e31083. doi: 10.2196/31083.
Sepsis is a significant cause of morbidity and mortality worldwide. Early detection of sepsis followed promptly by treatment initiation improves patient outcomes and saves lives. Hospitals are increasingly using computerized clinical decision support (CCDS) systems for the rapid identification of adult patients with sepsis.
This scoping review aims to systematically describe studies reporting on the use and evaluation of CCDS systems for the early detection of adult inpatients with sepsis.
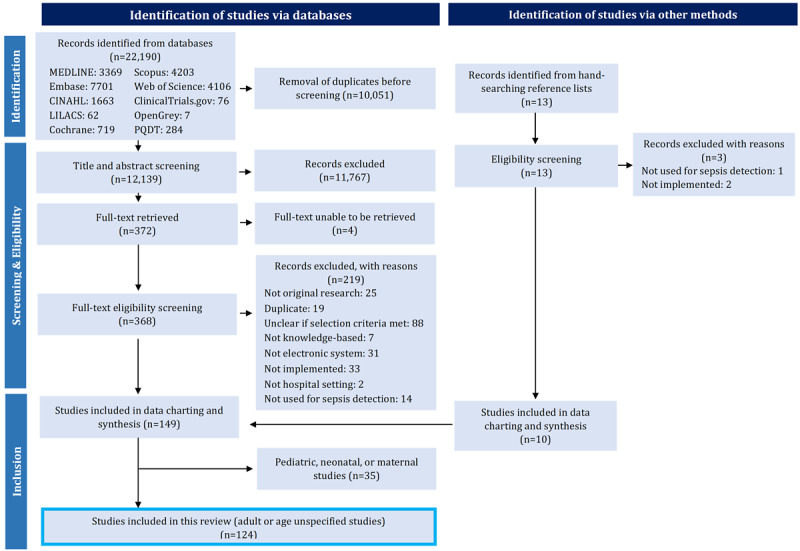
The protocol for this scoping review was previously published. A total of 10 electronic databases (MEDLINE, Embase, CINAHL, the Cochrane database, LILACS [Latin American and Caribbean Health Sciences Literature], Scopus, Web of Science, OpenGrey, ClinicalTrials.gov, and PQDT [ProQuest Dissertations and Theses]) were comprehensively searched using terms for sepsis, CCDS, and detection to identify relevant studies. Title, abstract, and full-text screening were performed by 2 independent reviewers using predefined eligibility criteria. Data charting was performed by 1 reviewer with a second reviewer checking a random sample of studies. Any disagreements were discussed with input from a third reviewer. In this review, we present the results for adult inpatients, including studies that do not specify patient age.
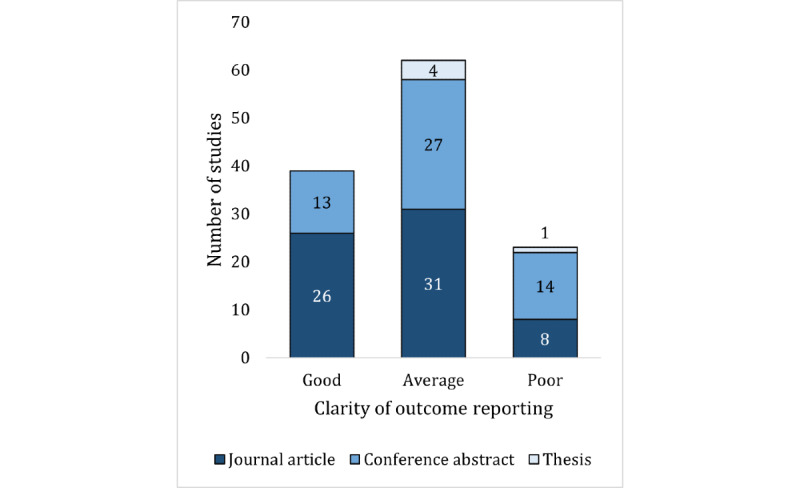
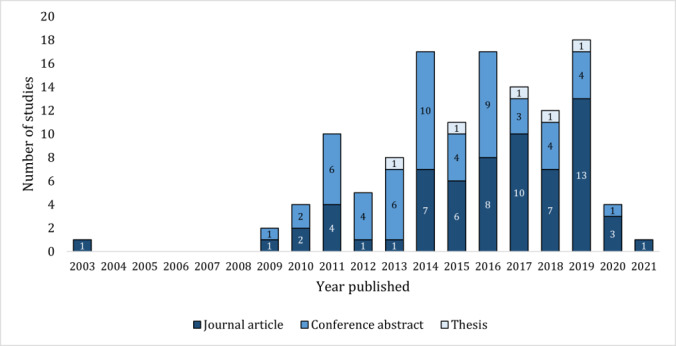
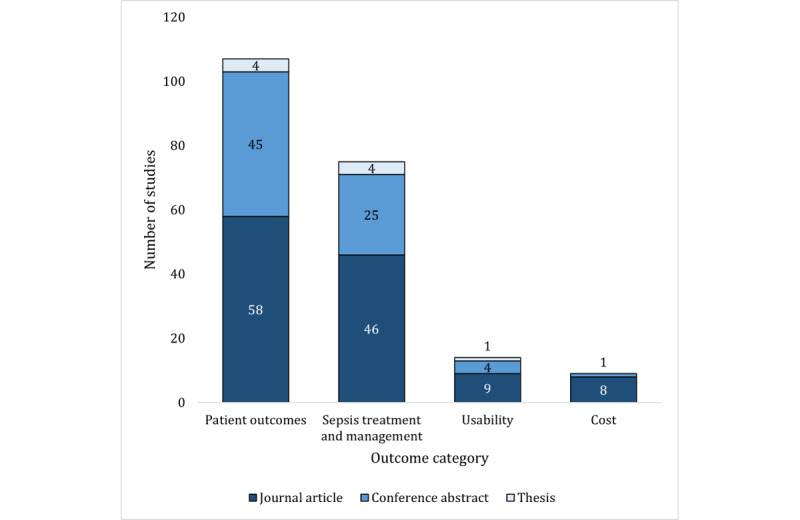
A search of the electronic databases retrieved 12,139 studies following duplicate removal. We identified 124 studies for inclusion after title, abstract, full-text screening, and hand searching were complete. Nearly all studies (121/124, 97.6%) were published after 2009. Half of the studies were journal articles (65/124, 52.4%), and the remainder were conference abstracts (54/124, 43.5%) and theses (5/124, 4%). Most studies used a single cohort (54/124, 43.5%) or before-after (42/124, 33.9%) approach. Across all 124 included studies, patient outcomes were the most frequently reported outcomes (107/124, 86.3%), followed by sepsis treatment and management (75/124, 60.5%), CCDS usability (14/124, 11.3%), and cost outcomes (9/124, 7.3%). For sepsis identification, the systemic inflammatory response syndrome criteria were the most commonly used, alone (50/124, 40.3%), combined with organ dysfunction (28/124, 22.6%), or combined with other criteria (23/124, 18.5%). Over half of the CCDS systems (68/124, 54.8%) were implemented alongside other sepsis-related interventions.
The current body of literature investigating the implementation of CCDS systems for the early detection of adult inpatients with sepsis is extremely diverse. There is substantial variability in study design, CCDS criteria and characteristics, and outcomes measured across the identified literature. Future research on CCDS system usability, cost, and impact on sepsis morbidity is needed.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): RR2-10.2196/24899.
败血症是全球发病率和死亡率的重要原因。及时发现败血症并迅速开始治疗可改善患者的预后并挽救生命。医院越来越多地使用计算机临床决策支持 (CCDS) 系统来快速识别成年败血症患者。
本范围综述旨在系统地描述报告用于早期检测成年住院患者败血症的 CCDS 系统的使用和评估的研究。
该范围综述的方案先前已发表。共综合检索了 10 个电子数据库(MEDLINE、Embase、CINAHL、Cochrane 数据库、LILACS[拉丁美洲和加勒比健康科学文献]、Scopus、Web of Science、OpenGrey、ClinicalTrials.gov 和 PQDT[ProQuest 学位论文和论文]),使用了败血症、CCDS 和检测的术语来确定相关研究。两名独立审查员使用预定义的纳入标准对标题、摘要和全文进行筛选。由一名评审员进行数据图表绘制,另一名评审员检查随机样本的研究。任何分歧都将在第三名评审员的参与下进行讨论。在本综述中,我们展示了针对成年住院患者的结果,包括未具体说明患者年龄的研究。
重复删除后,电子数据库的检索共检索到 12,139 篇研究。在标题、摘要和全文筛选以及手工搜索完成后,我们确定了 124 项符合纳入标准的研究。几乎所有研究(121/124,97.6%)都是在 2009 年后发表的。半数研究为期刊文章(65/124,52.4%),其余为会议摘要(54/124,43.5%)和论文(5/124,4%)。大多数研究使用单一队列(54/124,43.5%)或前后(42/124,33.9%)方法。在所有 124 项纳入研究中,患者结局是最常报告的结局(107/124,86.3%),其次是败血症治疗和管理(75/124,60.5%)、CCDS 可用性(14/124,11.3%)和成本结果(9/124,7.3%)。在败血症识别方面,全身炎症反应综合征标准是最常用的,单独使用(50/124,40.3%),与器官功能障碍联合使用(28/124,22.6%)或与其他标准联合使用(23/124,18.5%)。超过一半的 CCDS 系统(68/124,54.8%)与其他败血症相关干预措施同时实施。
目前研究使用 CCDS 系统早期检测成年败血症住院患者的文献非常多样化。在确定的文献中,研究设计、CCDS 标准和特征以及测量的结果存在很大差异。需要进一步研究 CCDS 系统的可用性、成本以及对败血症发病率的影响。
国际注册报告标识符(IRRID):RR2-10.2196/24899。