Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Centre for Infectious Disease Control, National Institute for Public Health and the Environment (RIVM), Bilthoven, The Netherlands.
BMC Med. 2022 Feb 24;20(1):97. doi: 10.1186/s12916-022-02300-9.
Rapid antigen diagnostic tests (Ag-RDTs) are the most widely used point-of-care tests for detecting SARS-CoV-2 infection. Since the accuracy may have altered by changes in SARS-CoV-2 epidemiology, indications for testing, sampling and testing procedures, and roll-out of COVID-19 vaccination, we evaluated the performance of three prevailing SARS-CoV-2 Ag-RDTs.
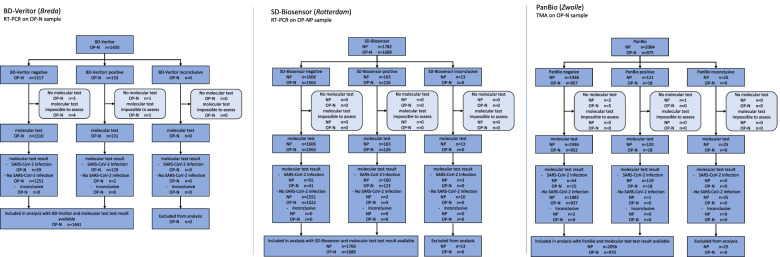
In this cross-sectional study, we consecutively enrolled individuals aged >16 years presenting for SARS-CoV-2 testing at three Dutch public health service COVID-19 test sites. In the first phase, participants underwent either BD-Veritor System (Becton Dickinson), PanBio (Abbott), or SD-Biosensor (Roche Diagnostics) testing with routine sampling procedures. In a subsequent phase, participants underwent SD-Biosensor testing with a less invasive sampling method (combined oropharyngeal-nasal [OP-N] swab). Diagnostic accuracies were assessed against molecular testing.
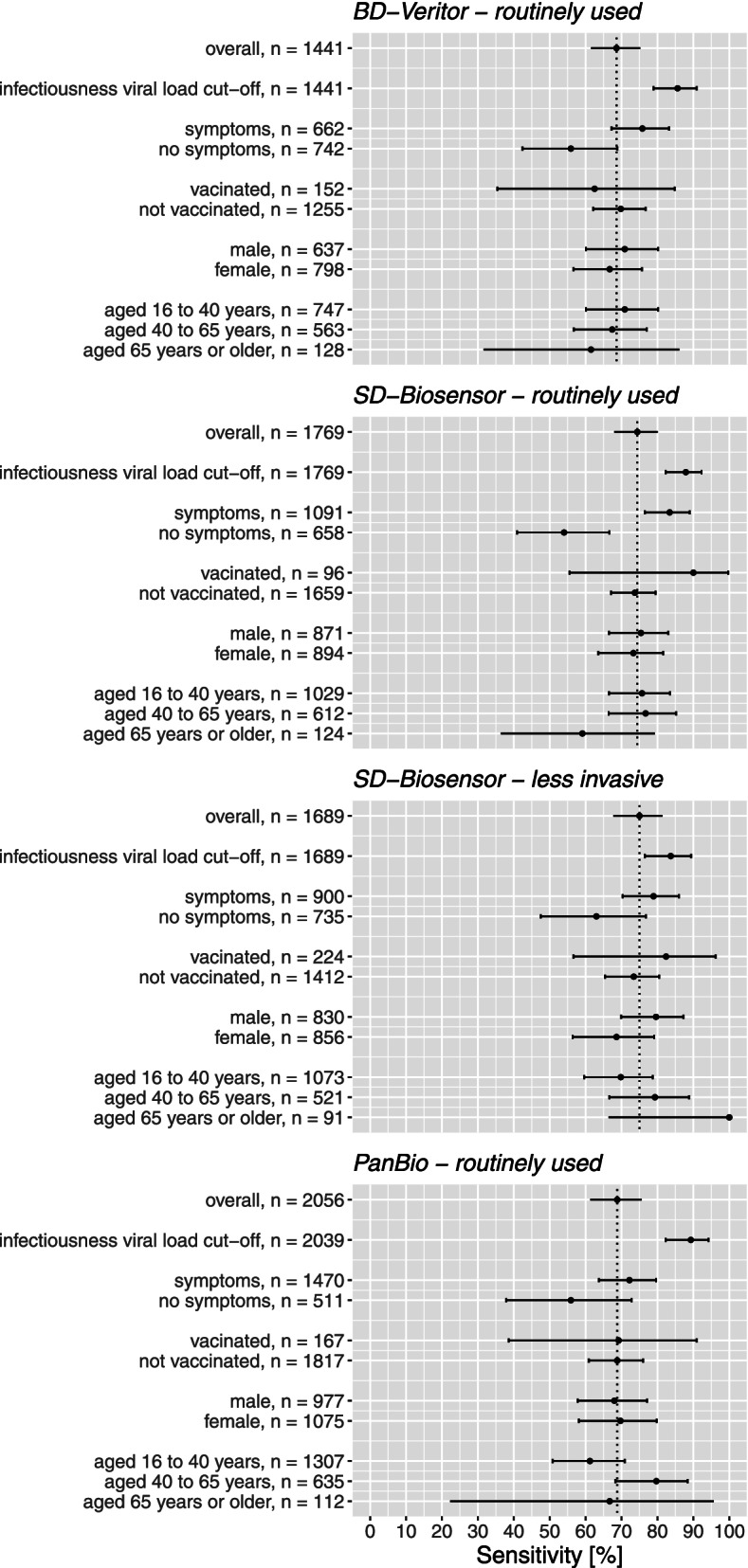
Six thousand nine hundred fifty-five of 7005 participants (99%) with results from both an Ag-RDT and a molecular reference test were analysed. SARS-CoV-2 prevalence and overall sensitivities were 13% (188/1441) and 69% (129/188, 95% CI 62-75) for BD-Veritor, 8% (173/2056) and 69% (119/173, 61-76) for PanBio, and 12% (215/1769) and 74% (160/215, 68-80) for SD-Biosensor with routine sampling and 10% (164/1689) and 75% (123/164, 68-81) for SD-Biosensor with OP-N sampling. In those symptomatic or asymptomatic at sampling, sensitivities were 72-83% and 54-56%, respectively. Above a viral load cut-off (≥5.2 log SARS-CoV-2 E-gene copies/mL), sensitivities were 86% (125/146, 79-91) for BD-Veritor, 89% (108/121, 82-94) for PanBio, and 88% (160/182, 82-92) for SD-Biosensor with routine sampling and 84% (118/141, 77-89) with OP-N sampling. Specificities were >99% for all tests in most analyses. Sixty-one per cent of false-negative Ag-RDT participants returned for testing within 14 days (median: 3 days, interquartile range 3) of whom 90% tested positive.
Overall sensitivities of three SARS-CoV-2 Ag-RDTs were 69-75%, increasing to ≥86% above a viral load cut-off. The decreased sensitivity among asymptomatic participants and high positivity rate during follow-up in false-negative Ag-RDT participants emphasise the need for education of the public about the importance of re-testing after an initial negative Ag-RDT should symptoms develop. For SD-Biosensor, the diagnostic accuracy with OP-N and deep nasopharyngeal sampling was similar; adopting the more convenient sampling method might reduce the threshold for professional testing.
快速抗原诊断检测(Ag-RDT)是目前最广泛用于检测 SARS-CoV-2 感染的即时检测方法。由于 SARS-CoV-2 的流行病学、检测指征、采样和检测程序以及 COVID-19 疫苗的推出发生了变化,因此我们评估了三种常用 SARS-CoV-2 Ag-RDT 的性能。
在这项横断面研究中,我们连续招募了在荷兰三个公共卫生服务 COVID-19 检测点因 SARS-CoV-2 检测就诊的年龄大于 16 岁的个体。在第一阶段,参与者接受了 BD-Veritor 系统(Becton Dickinson)、PanBio(Abbott)或 SD-Biosensor(罗氏诊断)检测,采用常规采样程序。在随后的阶段,参与者接受了 SD-Biosensor 检测,采用了一种侵入性较小的采样方法(联合鼻咽 [OP-N] 拭子)。通过分子检测评估诊断准确性。
对同时进行了 Ag-RDT 和分子参考检测的 7005 名参与者中的 6955 名(99%)的结果进行了分析。SARS-CoV-2 的流行率和总体敏感性分别为 BD-Veritor 的 13%(188/1441)和 69%(129/188,95%CI 62-75)、PanBio 的 8%(173/2056)和 69%(119/173,61-76)、SD-Biosensor 采用常规采样的 12%(215/1769)和 74%(160/215,68-80)和 SD-Biosensor 采用 OP-N 采样的 10%(164/1689)和 75%(123/164,68-81)。在有症状或无症状的个体中,敏感性分别为 72-83%和 54-56%。在病毒载量临界值(≥5.2 log SARS-CoV-2 E 基因拷贝/ml)以上,敏感性分别为 BD-Veritor 的 86%(125/146,79-91)、PanBio 的 89%(108/121,82-94)、SD-Biosensor 采用常规采样的 88%(160/182,82-92)和采用 OP-N 采样的 84%(118/141,77-89)。在大多数分析中,所有检测的特异性均大于 99%。61%的假阴性 Ag-RDT 参与者在 14 天内(中位数:3 天,四分位距 3)再次进行了检测,其中 90%的检测结果为阳性。
三种 SARS-CoV-2 Ag-RDT 的总体敏感性为 69-75%,在病毒载量临界值以上增加至≥86%。在无症状参与者中敏感性降低,以及假阴性 Ag-RDT 参与者在随访中高阳性率强调了公众需要了解在初始阴性 Ag-RDT 后出现症状时重新检测的重要性。对于 SD-Biosensor,采用 OP-N 和深鼻咽采样的诊断准确性相似;采用更方便的采样方法可能会降低专业检测的门槛。