Rheumatology Service, University Hospital Bellvitge, IDIBELL, Barcelona, Spain.
Rheumatology Service, University Hospital Virgen de la Arrixaca, Murcia, Spain.
Adv Ther. 2022 Apr;39(4):1490-1501. doi: 10.1007/s12325-022-02064-x. Epub 2022 Feb 24.
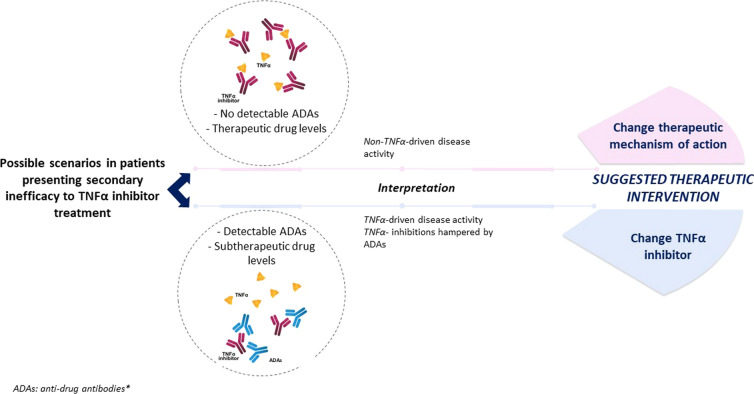
Axial spondyloarthritis is a chronic inflammatory rheumatic disease that affects the axial skeleton and causes severe pain and disability. It may be also associated with extra-articular manifestations. Early diagnosis and appropriate treatment can reduce the severity of the disease and the risk of progression. The biological disease-modifying antirheumatic drugs (bDMARDs) tumor necrosis factor alpha (TNFα) inhibitors (TNFi) and the anti-interleukin (IL)-17A antibodies secukinumab and ixekizumab are effective agents to reduce disease activity and minimize the inflammation that damages the joints. New alternatives such as Janus kinase (JAK) inhibitors are also available. Unfortunately, response rates to bDMARDs are far from optimal, and many patients experience so-called treatment failure. The definition of treatment failure definition is often vague and may depend on the rigorousness of the therapeutic goal, the inclusion or not of peripheral symptoms/extra-articular manifestations, or patients' overall health. After an exhaustive bibliographic review, we propose a definition based on loss of the following status: low disease activity assessed by Ankylosing Spondylitis Disease Activity Score (ASDAS)-CRP, absence of extra-articular manifestations, and low disease impact on the patients' general health. Apart from discontinuing the therapy because of safety or intolerance reasons, two types of treatment failure can be differentiated depending on when it occurs: primary failure (no response within 6 months after treatment initiation, or lack of efficacy) and secondary failure (response within 6 months but lost thereafter, or loss of efficacy over time). Physicians should carefully consider the moment and the reason for the treatment failure to decide the next therapeutic step. In the case of primary failure on a first TNFi, it seems reasonable to switch to another class of drugs, i.e., an anti-IL-17 agent, as phase III trials showed that the response to IL-17 blockade was higher than to placebo in patients previously exposed to TNFi. When secondary failure occurs, and loss of efficacy is suspected to be caused by antidrug antibodies (ADAs), it is advisable to analyze serum TNFi and ADAs concentrations, if possible; in the presence of ADAs and low TNFi levels, changing the TNFi is rational as it may restore the TNFα blocking capacity. If ADAs are absent/low with adequate drug therapeutic levels, switching to another target might be the best strategy.
中轴型脊柱关节炎是一种慢性炎症性风湿性疾病,影响中轴骨骼,导致严重疼痛和残疾。它也可能与关节外表现有关。早期诊断和适当的治疗可以降低疾病的严重程度和进展的风险。生物疾病修饰抗风湿药物(bDMARDs)肿瘤坏死因子 α(TNFα)抑制剂(TNFi)和抗白细胞介素(IL)-17A 抗体司库奇尤单抗和依奇珠单抗是减少疾病活动度和最小化炎症损伤关节的有效药物。新的替代药物如 Janus 激酶(JAK)抑制剂也可用。不幸的是,bDMARDs 的反应率远非理想,许多患者经历所谓的治疗失败。治疗失败的定义往往不明确,可能取决于治疗目标的严格程度、是否包括外周症状/关节外表现,或患者的整体健康状况。在对文献进行全面回顾后,我们提出了一个基于以下状态丧失的定义:通过强直性脊柱炎疾病活动评分(ASDAS-CRP)评估的低疾病活动度、无关节外表现以及疾病对患者整体健康状况的低影响。除了因安全性或不耐受原因而停止治疗外,根据其发生时间,可以将治疗失败分为两种类型:原发性失败(治疗开始后 6 个月内无反应,或无疗效)和继发性失败(6 个月内有反应但此后失去疗效,或随着时间的推移疗效丧失)。医生应仔细考虑治疗失败的时间和原因,以决定下一步的治疗方案。如果首次使用 TNFi 出现原发性失败,似乎可以合理地切换到另一类药物,即抗 IL-17 药物,因为 III 期试验表明,在先前暴露于 TNFi 的患者中,IL-17 阻断的反应高于安慰剂。当发生继发性失败且怀疑疗效丧失是由抗药抗体(ADA)引起时,最好分析血清 TNFi 和 ADA 浓度,如果可能的话;在存在 ADA 和低 TNFi 水平的情况下,更换 TNFi 是合理的,因为它可能恢复 TNFα 阻断能力。如果 ADA 缺失/低且药物治疗水平充足,切换到另一个靶点可能是最佳策略。