Autore Giovanni, Neglia Cosimo, Di Costanzo Margherita, Ceccoli Martina, Vergine Gianluca, La Scola Claudio, Malaventura Cristina, Falcioni Alice, Iacono Alessandra, Crisafi Antonella, Iughetti Lorenzo, Conte Maria Luisa, Pierantoni Luca, Gatti Claudia, Biasucci Giacomo, Esposito Susanna
Pediatric Clinic, Department of Medicine and Surgery, University of Parma, 43126 Parma, Italy.
Paediatrics and Neonatology Unit, Guglielmo da Saliceto Hospital, 29122 Piacenza, Italy.
Children (Basel). 2022 Jan 19;9(2):128. doi: 10.3390/children9020128.
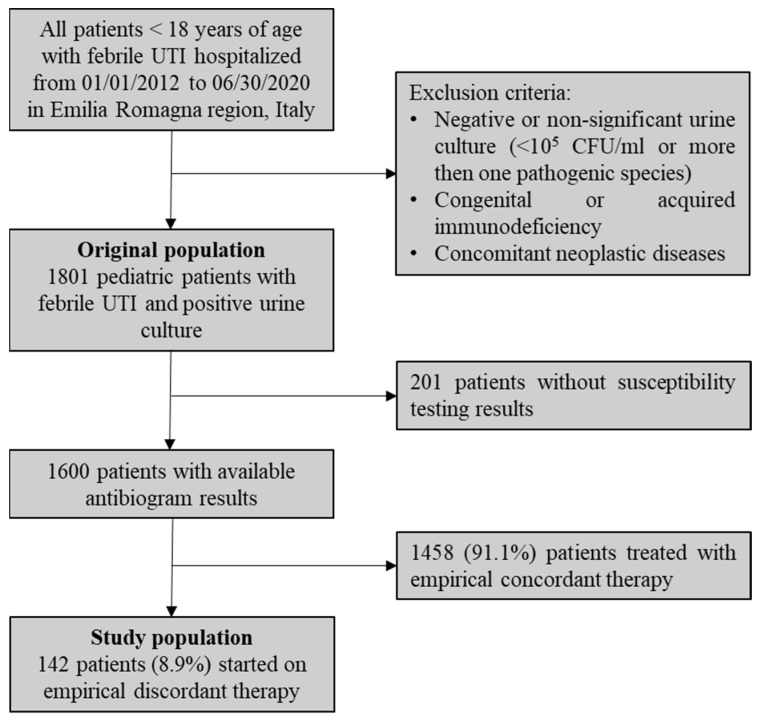
With the spread of antibiotic resistance in pediatric urinary tract infections (UTIs), more patients are likely to be started empirically on antibiotics to which pathogens are later found to be resistant (discordant therapy). However, in-vivo effectiveness may be different from in-vitro susceptibility. Aims of this study were to describe clinical outcomes of discordant empirical treatments in pediatric UTIs and to investigate risk factors associated to treatment failure. This observational, retrospective study was conducted on children hospitalized for febrile UTIs with positive urine culture and started on discordant empirical therapy. Failure rates of discordant treatments and associated risk factors were investigated. A total of 142/1600 (8.9%) patients were treated with inadequate empirical antibiotics. Clinical failure was observed in 67/142 (47.2%) patients, with no fatal events. Higher failure rates were observed for combinations of penicillin and beta-lactamase inhibitors (57.1%). Significant risk factors for failure of discordant treatment were history of recurrent UTIs (95% CI: 1.13-9.98, OR: 3.23, < 0.05), recent use of antibiotics (95% CI: 1.46-21.82, OR: 5.02, < 0.01), infections caused by (95% CI: 1.85-62.10, OR: 7.30, < 0.05), and empirical treatment with combinations of penicillin and beta-lactamase inhibitors (95% CI: 0.94-4.03, OR: 1.94, = 0.05). This study showed that discordant empirical treatments may still be effective in more than half of pediatric UTIs. Clinical effectiveness varies between different discordant antibiotics in pediatric UTIs, and patients presenting risk factors for treatment failure may need a differentiated empirical approach.
随着儿童尿路感染(UTIs)中抗生素耐药性的传播,越来越多的患者可能开始经验性使用抗生素,但后来发现病原体对这些抗生素耐药(不匹配治疗)。然而,体内有效性可能与体外敏感性不同。本研究的目的是描述儿童UTIs不匹配经验性治疗的临床结果,并调查与治疗失败相关的危险因素。这项观察性、回顾性研究针对因发热性UTIs住院且尿培养阳性并开始不匹配经验性治疗的儿童进行。研究了不匹配治疗的失败率及相关危险因素。共有142/1600(8.9%)的患者接受了不充分的经验性抗生素治疗。67/142(47.2%)的患者出现临床失败,无死亡事件。青霉素和β-内酰胺酶抑制剂联合使用的失败率更高(57.1%)。不匹配治疗失败的显著危险因素包括复发性UTIs病史(95%可信区间:1.13 - 9.98,比值比:3.23,<0.05)、近期使用抗生素(95%可信区间:1.46 - 21.82,比值比:5.02,<0.01)、由[此处原文缺失病原体相关内容]引起的感染(95%可信区间:1.85 - 62.10,比值比:7.30,<0.05)以及青霉素和β-内酰胺酶抑制剂联合经验性治疗(95%可信区间:0.94 - 4.03,比值比:1.94,=0.05)。本研究表明,超过一半的儿童UTIs不匹配经验性治疗可能仍然有效。儿童UTIs中不同不匹配抗生素的临床有效性有所不同,存在治疗失败危险因素的患者可能需要采用差异化的经验性治疗方法。