Bahadori Atessa, Kuhlmann Beatrice, Debray Dominique, Franchi-Abella Stephanie, Wacker Julie, Beghetti Maurice, Wildhaber Barbara E, McLin Valérie Anne
Pediatric Specialties Division, Department of Pediatrics, Gynecology, and Obstetrics, University Hospitals Geneva (HUG), University of Geneva, 1211 Geneva, Switzerland.
Pediatric Endocrinology, Cantonal Hospital Aarau, 5001 Aarau, Switzerland.
Children (Basel). 2022 Feb 11;9(2):243. doi: 10.3390/children9020243.
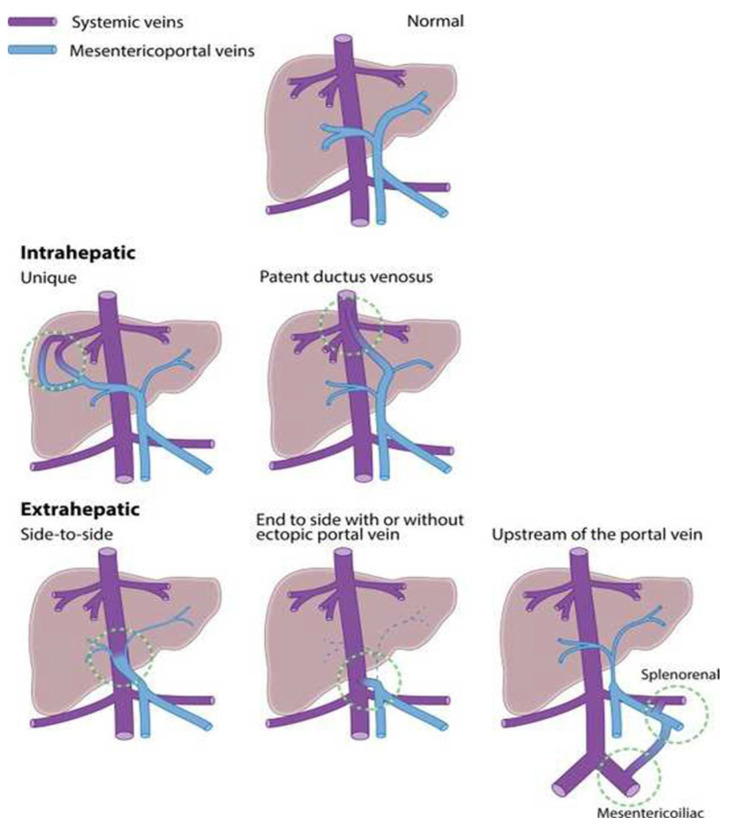
Congenital portosystemic shunts (CPSS) are rare vascular anomalies resulting in communications between the portal venous system and the systemic venous circulation, affecting an estimated 30,000 to 50,000 live births. CPSS can present at any age as a multi-system disease of variable severity mimicking both common and rare pediatric conditions.
Case A: A vascular malformation was identified in the liver of a 10-year-old girl with tall stature, advanced somatic maturation, insulin resistance with hyperinsulinemia, hyperandrogenemia and transient hematuria. Work-up also suggested elevated pulmonary pressures. Case B: A young girl with trisomy 8 mosaicism with a history of neonatal hypoglycemia, transient neonatal cholestasis and tall stature presented newly increased aminotransferase levels at 6 years of age. Case C: A 3-year-old boy with speech delay, tall stature and abdominal pain underwent abdominal ultrasound (US) showing multiple liver nodules, diagnosed as liver hemangiomas by hepatic magnetic resonance imaging (MRI). Management and outcome: After identification of a venous malformation on liver Doppler US, all three patients were referred to a specialized liver center for further work-up within 12 to 18 months from diagnosis. Angio-computed tomography (CT) scan confirmed the presence of either an intrahepatic or extrahepatic CPSS with multiples liver nodules. All three had a hyperintense signal in the globus pallidus on T1 weighted cerebral MRI. Right heart catheterization confirmed pulmonary hypertension in cases A and C. Shunts were closed either using an endovascular or surgical approach. Liver nodules were either surgically removed if there was a risk of malignant degeneration or closely monitored by serial imaging when benign.
These cases illustrate most of the common chief complaints and manifestations of CPSS. Liver Doppler US is the key to diagnosis. Considering portosystemic shunts in the diagnostic work-up of a patient with unexplained endocrine, liver, gastro-intestinal, cardiovascular, hematological, renal or neurocognitive disorder is important as prompt referral to a specialized center may significantly impact patient outcome.
先天性门体分流(CPSS)是一种罕见的血管异常,导致门静脉系统与体循环静脉之间出现交通,据估计每30000至50000例活产中会有1例受影响。CPSS可在任何年龄出现,表现为一种严重程度各异的多系统疾病,可模仿常见和罕见的儿科病症。
病例A:在一名10岁女孩的肝脏中发现了血管畸形,该女孩身材高大,身体发育早熟,存在胰岛素抵抗伴高胰岛素血症、高雄激素血症和短暂性血尿。检查还提示肺压力升高。病例B:一名患有8号染色体三体嵌合体的年轻女孩,有新生儿低血糖、短暂性新生儿胆汁淤积和身材高大的病史,在6岁时出现新的转氨酶水平升高。病例C:一名3岁男孩,有语言发育迟缓及身材高大和腹痛症状,接受腹部超声(US)检查显示肝脏有多个结节,肝脏磁共振成像(MRI)诊断为肝血管瘤。治疗与结果:在肝脏多普勒超声检查发现静脉畸形后,所有三名患者在确诊后的12至18个月内被转诊至专门的肝脏中心进行进一步检查。血管计算机断层扫描(CT)证实存在肝内或肝外CPSS以及多个肝脏结节。在T1加权脑MRI上,所有三人苍白球均有高信号。右心导管检查证实病例A和C存在肺动脉高压。通过血管内或手术方法关闭分流。如果存在恶性退变风险,对肝脏结节进行手术切除;如果为良性,则通过系列影像学检查密切监测。
这些病例说明了CPSS的大多数常见主要症状和表现。肝脏多普勒超声是诊断的关键。在对患有不明原因的内分泌、肝脏、胃肠道、心血管、血液、肾脏或神经认知障碍的患者进行诊断检查时,考虑门体分流很重要,因为及时转诊至专门中心可能会显著影响患者的预后。