Exley Mark A, Garcia Samantha, Zellander Amelia, Zilberberg Jenny, Andrews David W
Imvax, Inc., Philadelphia, PA 19602, USA.
Gastroenterology, Hepatology & Endoscopy, Brigham & Women's Hospital, Harvard Medical School, Boston, MA 02115, USA.
J Clin Med. 2022 Feb 18;11(4):1069. doi: 10.3390/jcm11041069.
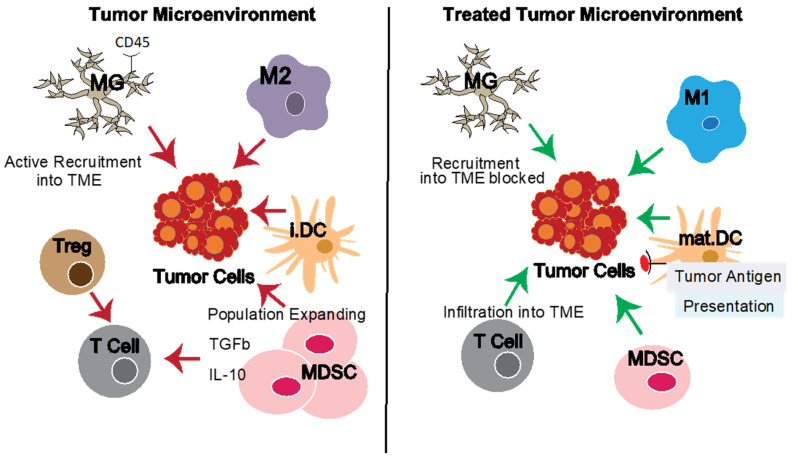
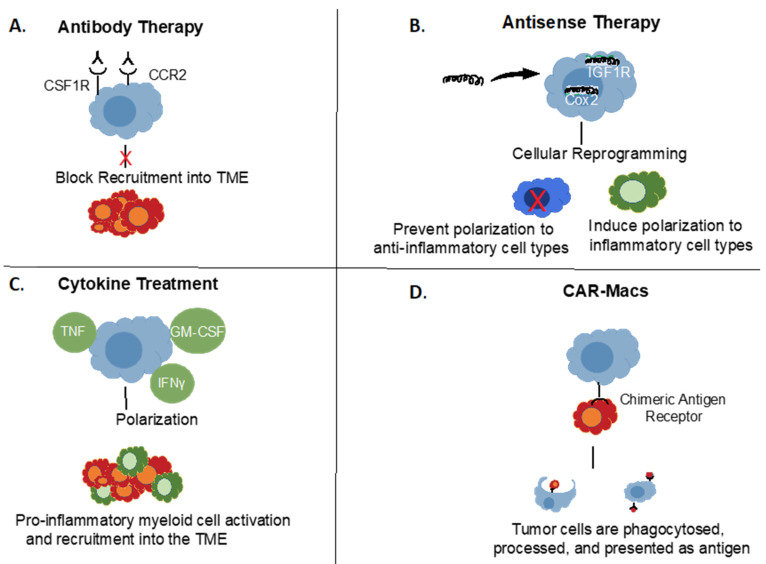
Glioblastoma multiforme (GBM), the most common and deadly brain cancer, exemplifies the paradigm that cancers grow with help from an immunosuppressive tumor microenvironment (TME). In general, TME includes a large contribution from various myeloid lineage-derived cell types, including (in the brain) altered pathogenic microglia as well as monocyte-macrophages (Macs), myeloid-derived suppressor cells (MDSC) and dendritic cell (DC) populations. Each can have protective roles, but has, by definition, been coopted by the tumor in patients with progressive disease. However, evidence demonstrates that myeloid immunosuppressive activities can be reversed in different ways, leading to enthusiasm for this therapeutic approach, both alone and in combination with potentially synergistic immunotherapeutic and other strategies. Here, we review the current understanding of myeloid cell immunosuppression of anti-tumor responses as well as potential targets, challenges, and developing means to reverse immunosuppression with various therapeutics and their status. Targets include myeloid cell colony stimulating factors (CSFs), insulin-like growth factor 1 (IGF1), several cytokines and chemokines, as well as CD40 activation and COX2 inhibition. Approaches in clinical development include antibodies, antisense RNA-based drugs, cell-based combinations, polarizing cytokines, and utilizing Macs as a platform for Chimeric Antigen Receptors (CAR)-based tumor targeting, like with CAR-T cells. To date, promising clinical results have been reported with several of these approaches.
多形性胶质母细胞瘤(GBM)是最常见且致命的脑癌,它体现了癌症在免疫抑制性肿瘤微环境(TME)的帮助下生长的模式。一般来说,TME很大程度上来自各种髓系谱系衍生的细胞类型,包括(在大脑中)发生改变的致病性小胶质细胞以及单核细胞 - 巨噬细胞(Macs)、髓系来源的抑制细胞(MDSC)和树突状细胞(DC)群体。每种细胞都可能具有保护作用,但根据定义,在患有进展性疾病的患者中,它们已被肿瘤利用。然而,有证据表明,髓系免疫抑制活性可以通过不同方式逆转,这引发了对这种治疗方法的热情,无论是单独使用还是与可能具有协同作用的免疫治疗及其他策略联合使用。在这里,我们回顾了目前对髓系细胞对抗肿瘤反应的免疫抑制作用的理解,以及潜在的靶点、挑战,以及通过各种治疗方法逆转免疫抑制的发展手段及其现状。靶点包括髓系细胞集落刺激因子(CSFs)、胰岛素样生长因子1(IGF1)、几种细胞因子和趋化因子,以及CD40激活和COX2抑制。临床开发中的方法包括抗体、基于反义RNA的药物、基于细胞的联合疗法、极化细胞因子,以及利用Macs作为基于嵌合抗原受体(CAR)的肿瘤靶向平台,就像CAR-T细胞一样。迄今为止,其中几种方法已报告了有前景的临床结果。