Department of Sociology, University of Ibadan, Ibadan, Nigeria.
Warwick Medical School, University of Warwick, Warwick, United Kingdom.
PLoS One. 2022 Feb 25;17(2):e0264725. doi: 10.1371/journal.pone.0264725. eCollection 2022.
Many urban residents in low- and middle-income countries live in unfavorable conditions with few healthcare facilities, calling to question the long-held view of urban advantage in health, healthcare access and utilization. We explore the patterns of healthcare utilization in these deprived neighborhoods by studying three such settlements in Nigeria.
The study was conducted in three slums in Southwestern Nigeria, categorized as migrant, indigenous or cosmopolitan, based on their characteristics. Using observational data of those who needed healthcare and used in-patient or out-patient services in the 12 months preceding the survey, frequencies, percentages and odds-ratios were used to show the study participants' environmental and population characteristics, relative to their patterns of healthcare use.
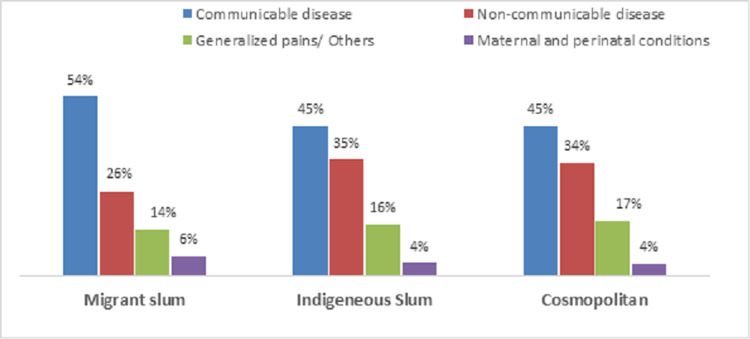
A total of 1,634 residents from the three slums participated, distributed as 763 (migrant), 459 (indigenous) and 412 (cosmopolitan). Residents from the migrant (OR = 0.70, 95%CI: 0.51 to 0.97) and indigenous (OR = 0.65, 95%CI: 0.45 to 0.93) slums were less likely to have used formal healthcare facilities than those from the cosmopolitan slum. Slum residents were more likely to use formal healthcare facilities for maternal and perinatal conditions, and generalized pains, than for communicable (OR = 0.50, 95%CI: 0.34 to 0.72) and non-communicable diseases (OR = 0.61, 95%CI: 0.41 to 0.91). The unemployed had higher odds (OR = 1.45, 95%CI: 1.08 to 1.93) of using formal healthcare facilities than those currently employed.
The cosmopolitan slum, situated in a major financial center and national economic hub, had a higher proportion of formal healthcare facility usage than the migrant and indigenous slums where about half of families were classified as poor. The urban advantage premise and Anderson behavioral model remain a practical explanatory framework, although they may not explain healthcare use in all possible slum types in Africa. A context-within-context approach is important for addressing healthcare utilization challenges in slums in sub-Saharan Africa.
许多中低收入国家的城市居民生活在条件不利的环境中,医疗设施匮乏,这对城市在健康、医疗保健可及性和利用方面具有优势的长期观点提出了质疑。我们通过研究尼日利亚的三个这样的定居点来探索这些贫困社区的医疗保健利用模式。
该研究在尼日利亚西南部的三个贫民窟进行,根据其特点将其分为移民、本土或国际化。使用调查前 12 个月需要医疗保健并使用门诊或住院服务的人的观察数据,使用频率、百分比和优势比来显示研究参与者的环境和人口特征,相对于他们的医疗保健使用模式。
共有来自三个贫民窟的 1634 名居民参与,其中 763 名(移民)、459 名(本土)和 412 名(国际化)。与国际化贫民窟的居民相比,移民(OR=0.70,95%CI:0.51 至 0.97)和本土(OR=0.65,95%CI:0.45 至 0.93)贫民窟的居民使用正规医疗设施的可能性较小。贫民窟居民更有可能因产妇和围产期疾病以及一般性疼痛而使用正规医疗设施,而不是因传染病(OR=0.50,95%CI:0.34 至 0.72)和非传染病(OR=0.61,95%CI:0.41 至 0.91)而使用正规医疗设施。失业者比目前就业者使用正规医疗设施的可能性更高(OR=1.45,95%CI:1.08 至 1.93)。
位于主要金融中心和国家经济中心的国际化贫民窟使用正规医疗设施的比例高于移民和本土贫民窟,其中约一半家庭被归类为贫困家庭。尽管城市优势前提和安德森行为模型可能无法解释非洲所有可能的贫民窟类型中的医疗保健使用情况,但它们仍然是一个实用的解释框架。在撒哈拉以南非洲的贫民窟中,需要采用情境内情境方法来解决医疗保健利用方面的挑战。