Wu Cheng-Kun, Chen Li-Wei, Chang Te-Sheng, Tung Shui-Yi, Lin Chun-Yen, Hung Chao-Hung, Lu Sheng-Nan, Lin Chih-Lang, Chen Chien-Hung, Hsu Chao-Wei, Hu Tsung-Hui, Sheen I-Shyan
Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung 83301, Taiwan.
Division of Hepato-Gastroenterology, Department of Internal Medicine, Keelung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Keelung 20420, Taiwan.
Viruses. 2022 Feb 10;14(2):362. doi: 10.3390/v14020362.
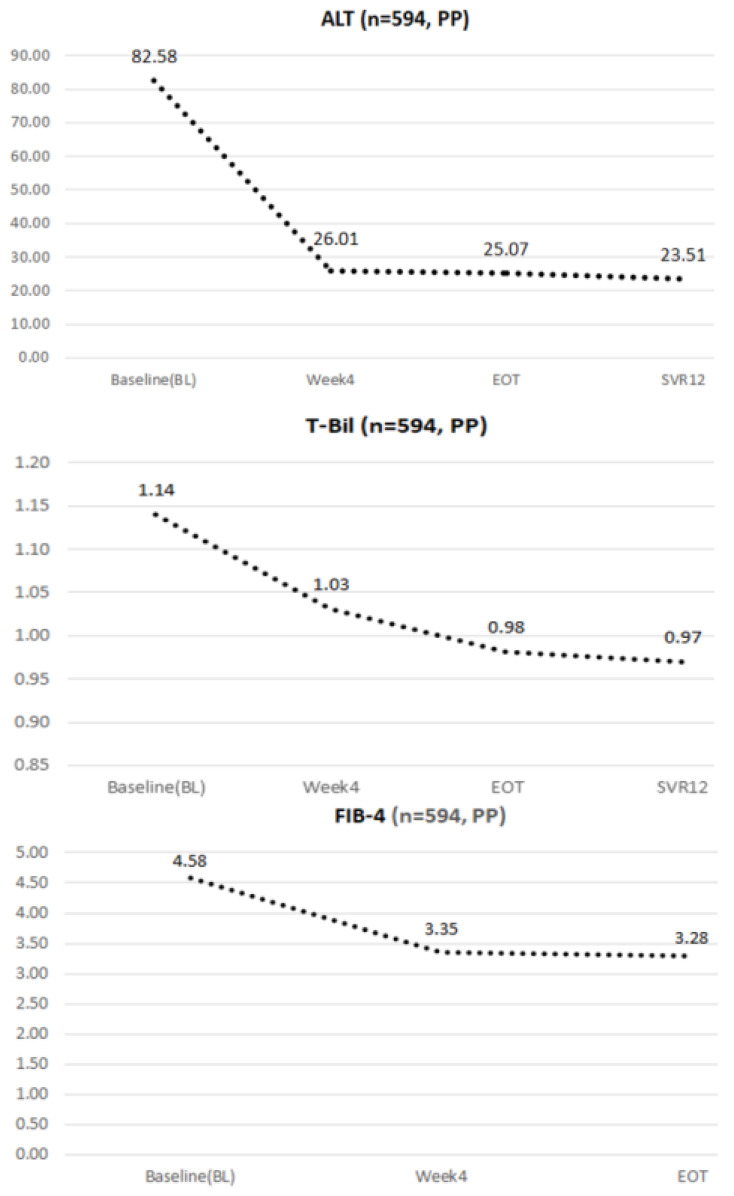
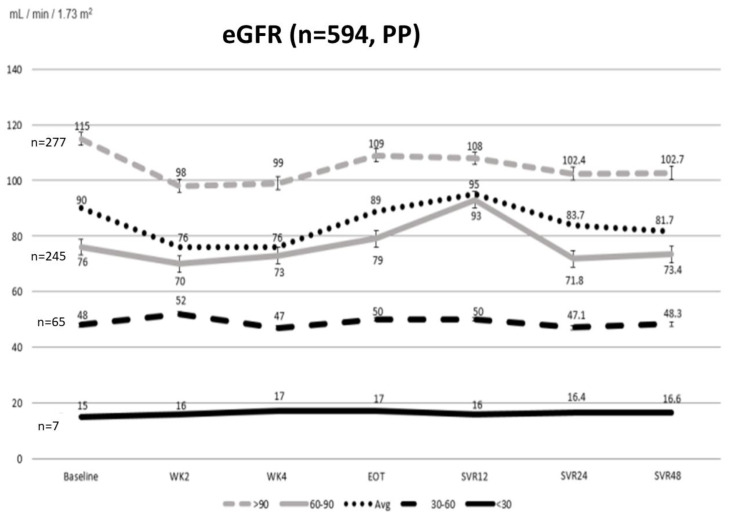
The results of long-term renal evolution in HCV-infected patients using sofosbuvir and velpatasvir (SOF/VEL), with or without ribavirin (RBV), are lacking. We evaluated the renal safety for HCV-infected patients receiving SOF/VEL. Between 1 June 2019 and 6 July 2020, we included 594 HCV-infected patients receiving SOF/VEL +/- RBV for 12 weeks in Taiwan. Viral eradication rate (defined by sustained virological response at week 12 post-treatment; SVR12) and changes to renal function were considered. SVR12 was achieved in 99.3% (590/594) upon per-protocol analysis. Patients saw improved hepatobiliary function and fibrosis after the start of SOF/VEL therapy. For renal function, those with baseline estimated glomerular filtration rate (eGFR) ≥ 60 (mL/min/1.73 m) experienced transient on-treatment reduction in renal function that improved upon ending treatment, but recurrent eGFR degradation during one-year follow-up. The use of RBV (OR = 5.200, 95% CI: 1.983-13.634, = 0.001) was a significant risk factor at SVR24, while diabetes mellitus (OR = 2.765, 95% CI: 1.104-6.922, = 0.030) and the use of RBV (OR = 3.143, 95% CI: 1.047-9.435, = 0.041) were identified as significant risk factors of worsening renal function at SVR48. SOF/VEL did not worsen renal function among those with stage 4-5 chronic kidney disease (CKD) who were not receiving dialysis. A trend of decline in eGFR at 1 year after SOF/VEL treatment was observed among diabetic patients with baseline eGFR ≥ 60 (mL/min/1.73 m) and concomitant use of RBV. The close monitoring of renal function is warranted. Further study should be conducted in order to weigh the risks and benefit of RBV.
目前尚缺乏关于使用索磷布韦和维帕他韦(SOF/VEL),无论是否联合利巴韦林(RBV)治疗丙型肝炎病毒(HCV)感染患者的长期肾脏转归情况。我们评估了接受SOF/VEL治疗的HCV感染患者的肾脏安全性。在2019年6月1日至2020年7月6日期间,我们纳入了台湾地区594例接受SOF/VEL±RBV治疗12周的HCV感染患者。研究考量了病毒根除率(定义为治疗后第12周持续病毒学应答;SVR12)以及肾功能变化。根据符合方案分析,99.3%(590/594)的患者实现了SVR12。患者在开始SOF/VEL治疗后,肝胆功能和纤维化情况有所改善。对于肾功能,基线估算肾小球滤过率(eGFR)≥60(mL/min/1.73 m²)的患者在治疗期间肾功能出现短暂下降,治疗结束后有所改善,但在一年随访期间eGFR再次下降。在SVR24时,使用RBV(比值比[OR]=5.200,95%置信区间[CI]:1.983 - 13.634,P=0.001)是一个显著的危险因素,而在SVR48时,糖尿病(OR = 2.765,95% CI:1.104 - 6.922,P = 0.030)和使用RBV(OR = 3.143,95% CI:1.047 - 9.435,P = 0.041)被确定为肾功能恶化的显著危险因素。对于未接受透析的4 - 5期慢性肾脏病(CKD)患者,SOF/VEL并未使肾功能恶化。在基线eGFR≥60(mL/min/1.73 m²)且同时使用RBV的糖尿病患者中,观察到SOF/VEL治疗1年后eGFR有下降趋势。有必要密切监测肾功能。应开展进一步研究以权衡RBV的风险和益处。