Zimmermann Paul, Moser Othmar, Edelmann Frank, Schöffl Volker, Eckstein Max L, Braun Martin
Department of Cardiology, Klinikum Bamberg, Bamberg, Germany.
Interdisciplinary Center of Sportsmedicine Bamberg, Klinikum Bamberg, Bamberg, Germany.
Front Physiol. 2022 Feb 11;13:739753. doi: 10.3389/fphys.2022.739753. eCollection 2022.
We analyzed data of 27 professional basketball players to prove cardiac remodeling referring echocardiographic parameters, cardiopulmonary exercise testing (CPET), and 12-lead electrocardiogram (ECG) analyses. The aim of our study was to present different characteristics in the athletes, on the one hand signs of a high vagal tone in the 12-lead ECG as criteria of early repolarization (ER), furthermore echocardiographic remodeling parameters and finally the performance in CPET. Therefore, we divided the cohort into a group with signs of ER pattern in the 12-lead ECG and without these criteria and presented the differences in detail.
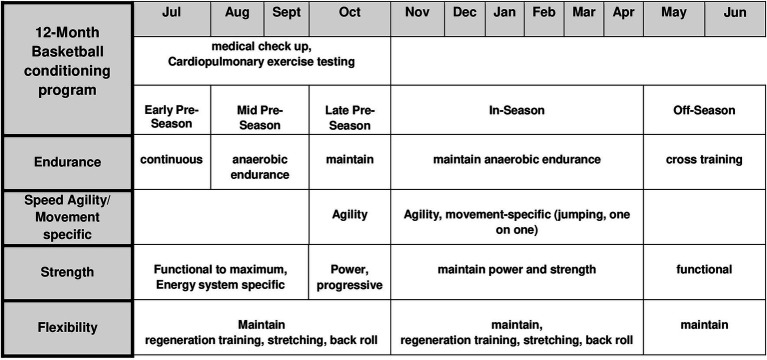
This was a single-center, retrospective study performed in 27 professional basketball players (age: 26.5 ± 7.5 years, male: 27, height: 197.2 ± 12 cm, weight: 100 ± 17 kg, BMI: 25.7 ± 3.4 kg/m). All participants underwent a sports medicine checkup, ECG analysis, transthoracic echocardiographic examination, and a CPET on a cycle ergometer between 2015 and 2019 during their pre-season preparation time. All individuals were healthy people without cardiological advance anamnesis. After assessment, two groups were built based on electrocardiographic criteria of ER pattern and a group without these criteria and compared against each other for parameters of echocardiographic assessment, CPET, and 12-lead ECG analysis. Data were analyzed with Minitab statistic program (Minitab Inc., State College, PA, United States) and Graph Pad Prism 8.2.1 (279; Graph Pad Software, San Diego, CA, United States) using ANOVA testing with testing and unpaired t-testing ( ≤ 0.05).Retrospectively additional information was collected referring to the management of training sessions, recovery time, and nutrition by interviewing the athletic training staff in order to understand the principles for individual athlete's training management and physiological and cardiopulmonary interactions.
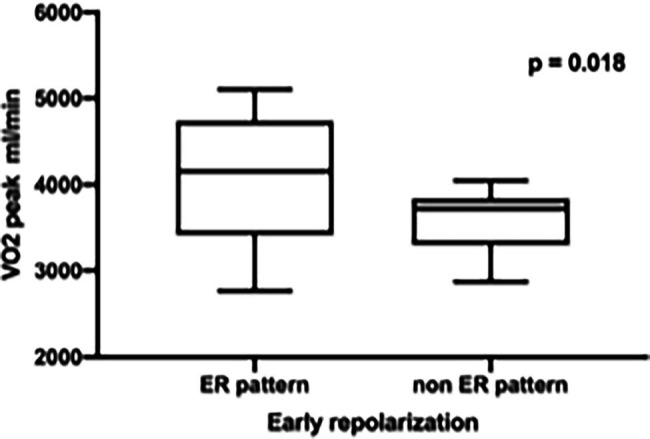
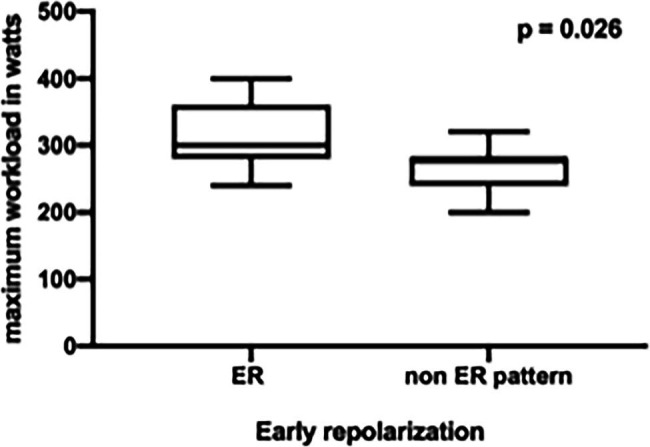
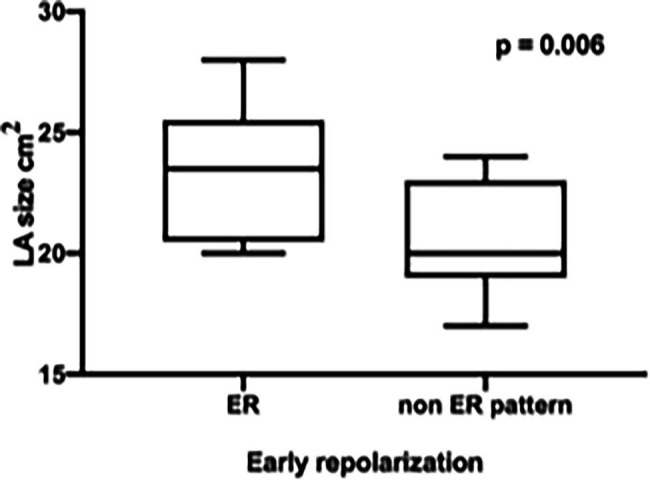
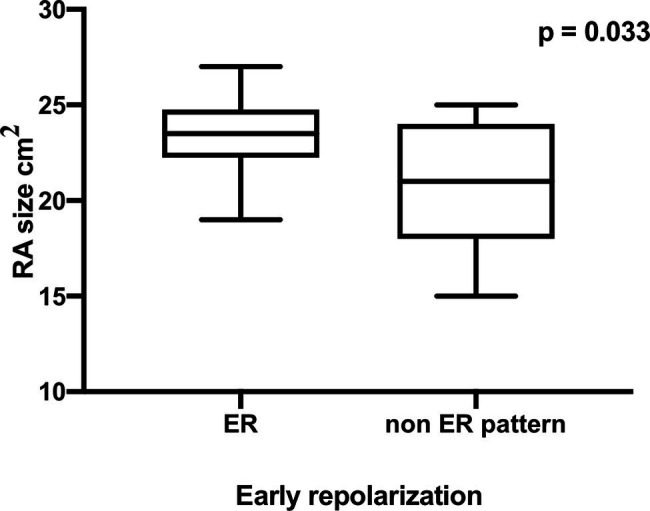
Comparing professional basketball players with ER pattern to those with no ER pattern, significant differences were found for CPET, echocardiographic, and ECG analysis ( < 0.05). Absolute and relativized peak oxygen uptake (VO; ER 4120 ± 750 ml/min (39 ± 5.4 ml/kg/min) vs. non-ER 3556 ± 393 ml/min (37.2 ± 5.3 ml/kg/min), = 0.018) and maximum workload during CPET (ER 310 ± 51.5 Watt (2.94 ± 0.35 W/kg) vs. non-ER 271 ± 32 Watt (2.85 ± 0.49 W/kg), = 0.026) was higher in athletes with an ER pattern. Furthermore, ER pattern athletes showed a higher enddiastolic left ventricular diameter (LVedd; ER 58.3 ± 7.9 mm vs. non-ER 53.6 ± 3.6 mm, = 0.048) and a significantly enlarged left atrial (LA) endsystolic diameter (ER 23.33 ± 2.71 mm vs. non-ER 20.47 ± 2.29 mm, = 0.006) as well as a significantly enlarged right atrial (RA) endsystolic diameter (ER 23.42 ± 2.15 mm vs. non-ER 20.93 ± 3.28 mm, = 0.033). Significant differences between the two compared groups could be revealed for left ventricular mass Index (LVMI gr/m; LVMI ER 113 gr/m ± 17.5 vs. LVMI non-ER 91.3 gr/m ± 15.1, = 0.002), but no significant differences for the relative wall thickness were found (RWT; RWT ER 0.49 ± 0.11 vs. RWT non-ER 0.38 ± 0.06, = 0.614).
Professional basketball players with criteria of ER pattern showed different results in CPET and cardiac remodeling as athletes with no ER pattern. These findings should encourage the athletic training staff to emphasize the quality of an individual training schedule for each athlete based on the cardiopulmonary pre-season sport medicine checkup. Nevertheless, echocardiographic findings, ER pattern, and performance in CPET have to be interpreted referring the sport-specific and athlete's ethnical background.
我们分析了27名职业篮球运动员的数据,通过超声心动图参数、心肺运动试验(CPET)和12导联心电图(ECG)分析来证明心脏重塑。我们研究的目的是呈现运动员的不同特征,一方面是12导联心电图中高迷走神经张力的迹象作为早期复极(ER)的标准,此外还有超声心动图重塑参数,最后是CPET中的表现。因此,我们将该队列分为在12导联心电图中有ER模式迹象的组和没有这些标准的组,并详细呈现了差异。
这是一项在27名职业篮球运动员(年龄:26.5±7.5岁,男性:27名,身高:197.2±12厘米,体重:100±17千克,BMI:25.7±3.4千克/米)中进行的单中心回顾性研究。所有参与者在2015年至2019年季前准备期间接受了运动医学检查、心电图分析、经胸超声心动图检查以及在自行车测力计上进行的CPET。所有个体均为无心脏病史的健康人。评估后,根据ER模式的心电图标准建立了两组,一组有这些标准,另一组没有,并针对超声心动图评估参数、CPET和12导联心电图分析进行相互比较。使用Minitab统计程序(美国宾夕法尼亚州立大学公园市的Minitab公司)和Graph Pad Prism 8.2.1(279;美国加利福尼亚州圣地亚哥的Graph Pad软件公司)进行数据分析,采用方差分析测试以及检验和非配对t检验(≤0.05)。通过采访运动训练人员,回顾性收集了有关训练课程管理、恢复时间和营养的其他信息,以便了解个体运动员训练管理的原则以及生理和心肺相互作用。
将有ER模式的职业篮球运动员与无ER模式的运动员进行比较,发现CPET、超声心动图和心电图分析存在显著差异(<0.05)。有ER模式的运动员的绝对和相对峰值摄氧量(VO;ER为4120±750毫升/分钟(39±5.4毫升/千克/分钟),无ER为3556±393毫升/分钟(37.2±5.3毫升/千克/分钟),=0.018)以及CPET期间的最大工作量(ER为310±51.5瓦特(2.94±0.35瓦/千克),无ER为271±32瓦特(2.85±0.49瓦/千克),=0.026)更高。此外,有ER模式的运动员表现出更高的舒张末期左心室直径(LVedd;ER为58.3±7.9毫米,无ER为53.6±3.6毫米,=0.048)以及显著增大的左心房(LA)收缩末期直径(ER为23.33±2.71毫米,无ER为20.47±2.29毫米,=0.006)以及显著增大的右心房(RA)收缩末期直径(ER为23.42±2.15毫米,无ER为20.93±3.28毫米,=0.033)。两组之间在左心室质量指数(LVMI克/米;LVMI ER为113克/米±17.5,LVMI无ER为91.3克/米±15.1,=0.002)方面存在显著差异,但在相对壁厚度方面未发现显著差异(RWT;RWT ER为0.49±0.11,RWT无ER为0.38±0.06,=0.614)。
有ER模式标准的职业篮球运动员在CPET和心脏重塑方面与无ER模式的运动员表现出不同的结果。这些发现应鼓励运动训练人员根据心肺季前运动医学检查,强调为每位运动员制定个性化训练计划的质量。然而,超声心动图结果、ER模式和CPET表现必须结合运动项目特点和运动员的种族背景进行解读。