Hu Rixin, Tao Tao, Yu Lu, Ding Qiuxia, Zhu Guanghui, Peng Guoyu, Zheng Shiwen, Yang Leyun, Wu Song
Health Science Center, School of Basic Medical Sciences, Shenzhen University, Shenzhen, China.
Department of Urology, The Affiliated Luohu Hospital of Shenzhen University, Shenzhen University, Shenzhen, China.
Front Cell Dev Biol. 2022 Feb 9;9:809588. doi: 10.3389/fcell.2021.809588. eCollection 2021.
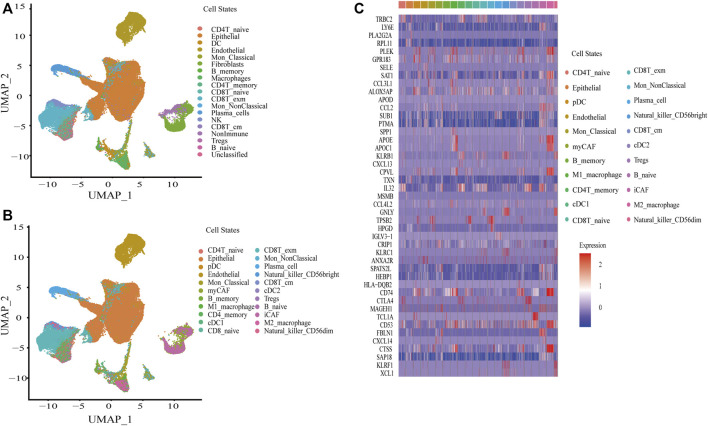
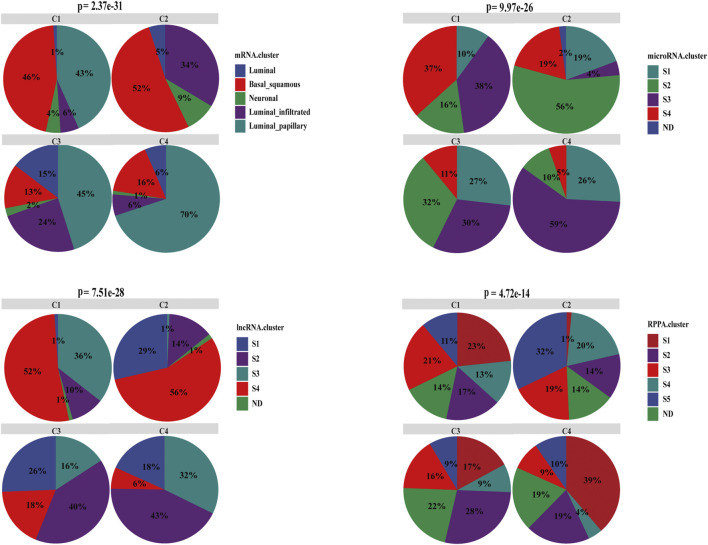
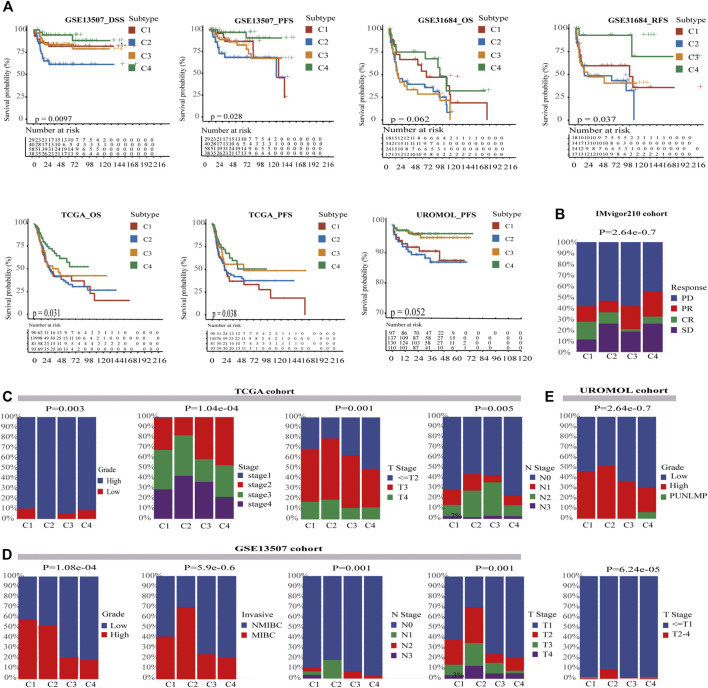
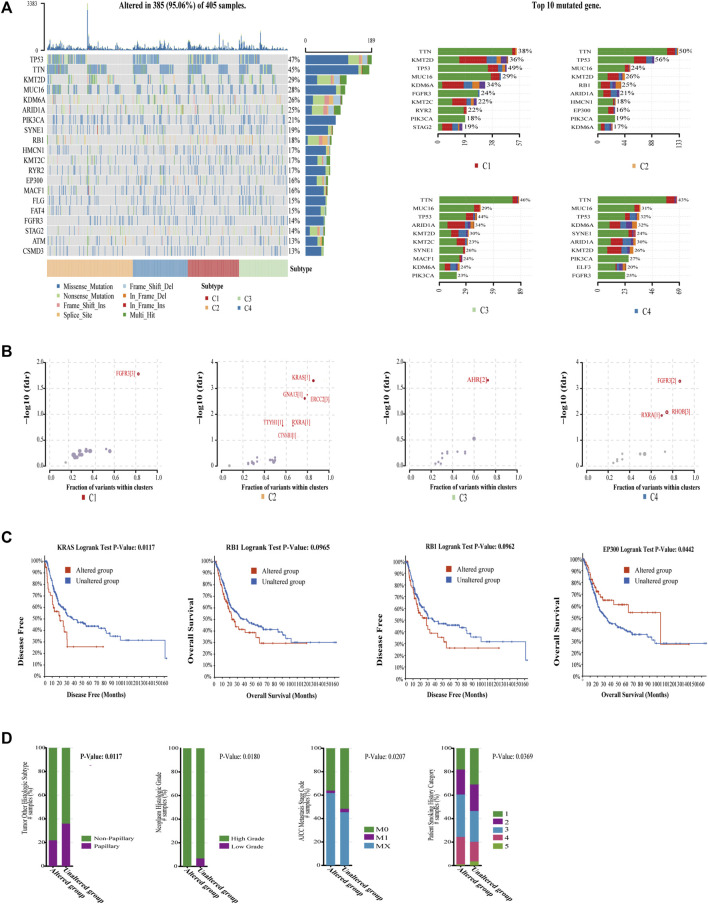
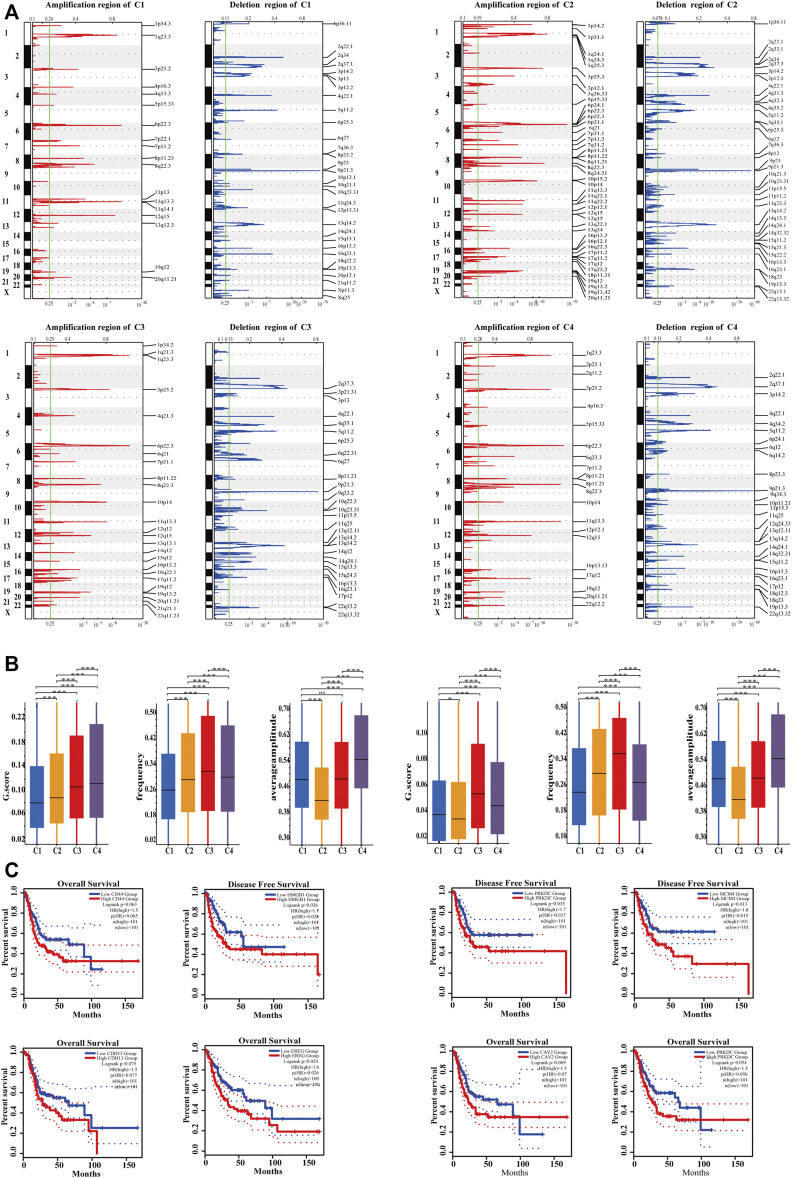
Due to the strong heterogeneity of bladder cancer (BC), there is often substantial variation in the prognosis and efficiency of immunotherapy among BC patients. For the precision treatment and assessment of prognosis, the subtyping of BC plays a critical role. Despite various subtyping methods proposed previously, most of them are based on a limited number of molecules, and none of them is developed on the basis of cell states. In this study, we construct a single-cell atlas by integrating single cell RNA-seq, RNA microarray, and bulk RNA-seq data to identify the absolute proportion of 22 different cell states in BC, including immune and nonimmune cell states derived from tumor tissues. To explore the heterogeneity of BC, BC was identified into four different subtypes in multiple cohorts using an improved consensus clustering algorithm based on cell states. Among the four subtypes, C1 had median prognosis and best overall response rate (ORR), which characterized an immunosuppressive tumor microenvironment. C2 was enriched in epithelial-mesenchymal transition/invasion, angiogenesis, immunosuppression, and immune exhaustion. Surely, C2 performed the worst in prognosis and ORR. C3 with worse ORR than C2 was enriched in angiogenesis and almost nonimmune exhaustion. Displaying an immune effective environment, C4 performed the best in prognosis and ORR. We found that patients with just an immunosuppressive environment are suitable for immunotherapy, but patients with an immunosuppressive environment accompanied by immune exhaustion or angiogenesis may resist immunotherapy. Furthermore, we conducted exploration into the heterogeneity of the transcriptome, mutational profiles, and somatic copy-number alterations in four subtypes, which could explain the significant differences related to cell states in prognosis and ORR. We also found that PD-1 in immune and tumor cells could both influence ORR in BC. The level of TGFβ in a cell state can be opposite to the overall level in the tissues, and the level in a specific cell state could predict ORR more accurately. Thus, our work furthers the understanding of heterogeneity and immunotherapy resistance in BC, which is expected to assist clinical practice and serve as a supplement to the current subtyping method from a novel perspective of cell states.
由于膀胱癌(BC)具有很强的异质性,BC患者的预后和免疫治疗效果往往存在很大差异。对于精准治疗和预后评估,BC的亚型分类起着关键作用。尽管此前提出了各种亚型分类方法,但大多数都是基于有限数量的分子,而且没有一种是基于细胞状态开发的。在本研究中,我们通过整合单细胞RNA测序、RNA微阵列和批量RNA测序数据构建了一个单细胞图谱,以确定BC中22种不同细胞状态的绝对比例,包括源自肿瘤组织的免疫和非免疫细胞状态。为了探究BC的异质性,我们使用基于细胞状态的改进共识聚类算法在多个队列中将BC分为四种不同亚型。在这四种亚型中,C1的预后中等,总体缓解率(ORR)最佳,其特征是免疫抑制性肿瘤微环境。C2富含上皮-间质转化/侵袭、血管生成、免疫抑制和免疫耗竭。当然,C2的预后和ORR最差。C3的ORR比C2差,富含血管生成且几乎没有免疫耗竭。C4表现出免疫有效环境,预后和ORR最佳。我们发现,仅具有免疫抑制环境的患者适合免疫治疗,但伴有免疫耗竭或血管生成的免疫抑制环境患者可能对免疫治疗有抗性。此外,我们对四种亚型中的转录组、突变谱和体细胞拷贝数改变的异质性进行了探究,这可以解释与细胞状态相关的预后和ORR的显著差异。我们还发现,免疫细胞和肿瘤细胞中的PD-1都可以影响BC的ORR。细胞状态下的TGFβ水平可能与组织中的总体水平相反,特定细胞状态下的水平可以更准确地预测ORR。因此,我们的工作进一步加深了对BC异质性和免疫治疗抗性的理解,有望辅助临床实践,并从细胞状态的新角度为当前的亚型分类方法提供补充。