University of Groningen, Department of Cardiology, University Medical Center Groningen, The Netherlands (I.E.B., C.S.P.L., A.A.V., J.M.t.M., K.D.).
National Heart Centre Singapore and Duke-National University of Singapore (C.S.P.L.).
Circulation. 2022 Mar;145(9):693-712. doi: 10.1161/CIRCULATIONAHA.121.052792. Epub 2022 Feb 28.
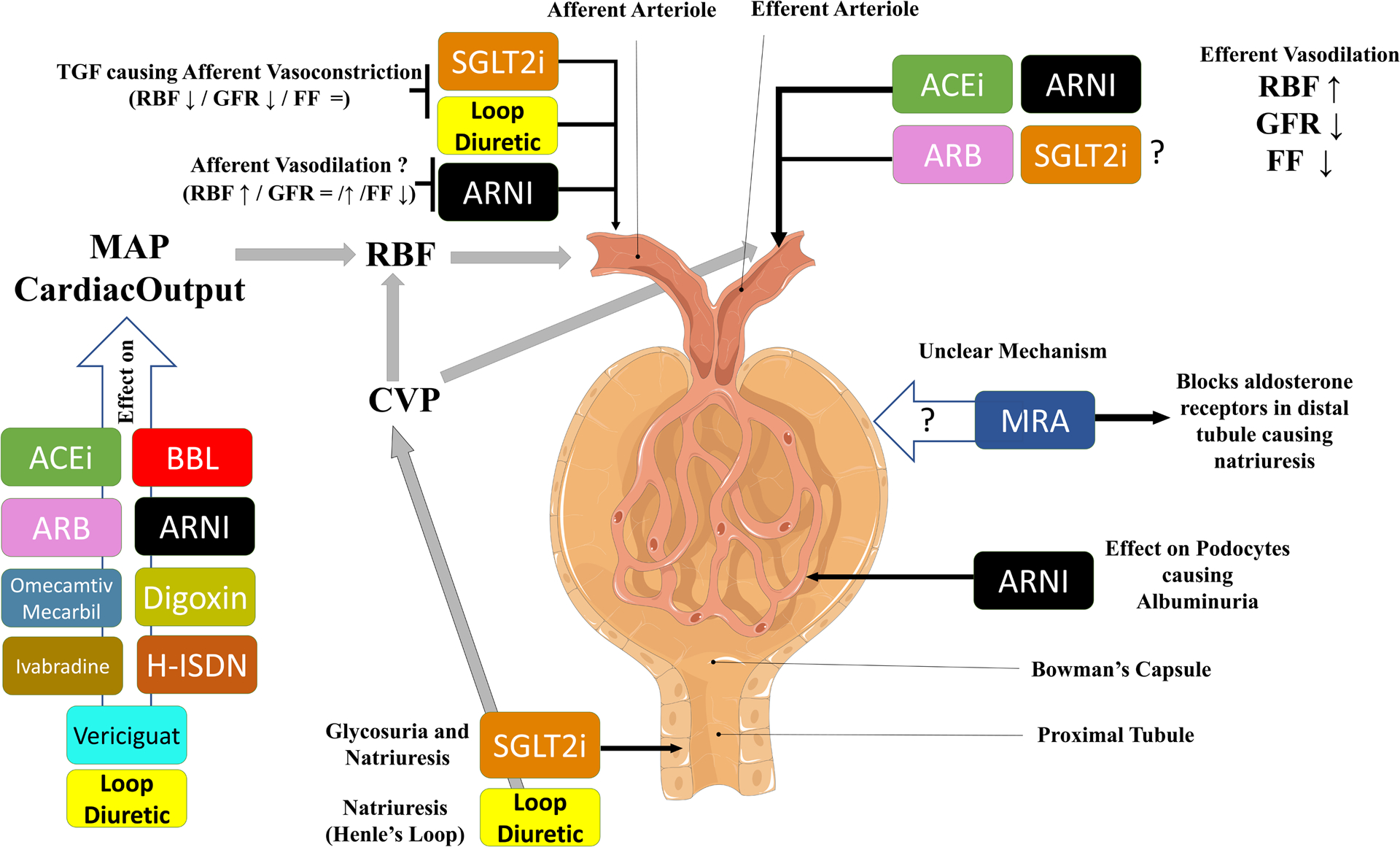
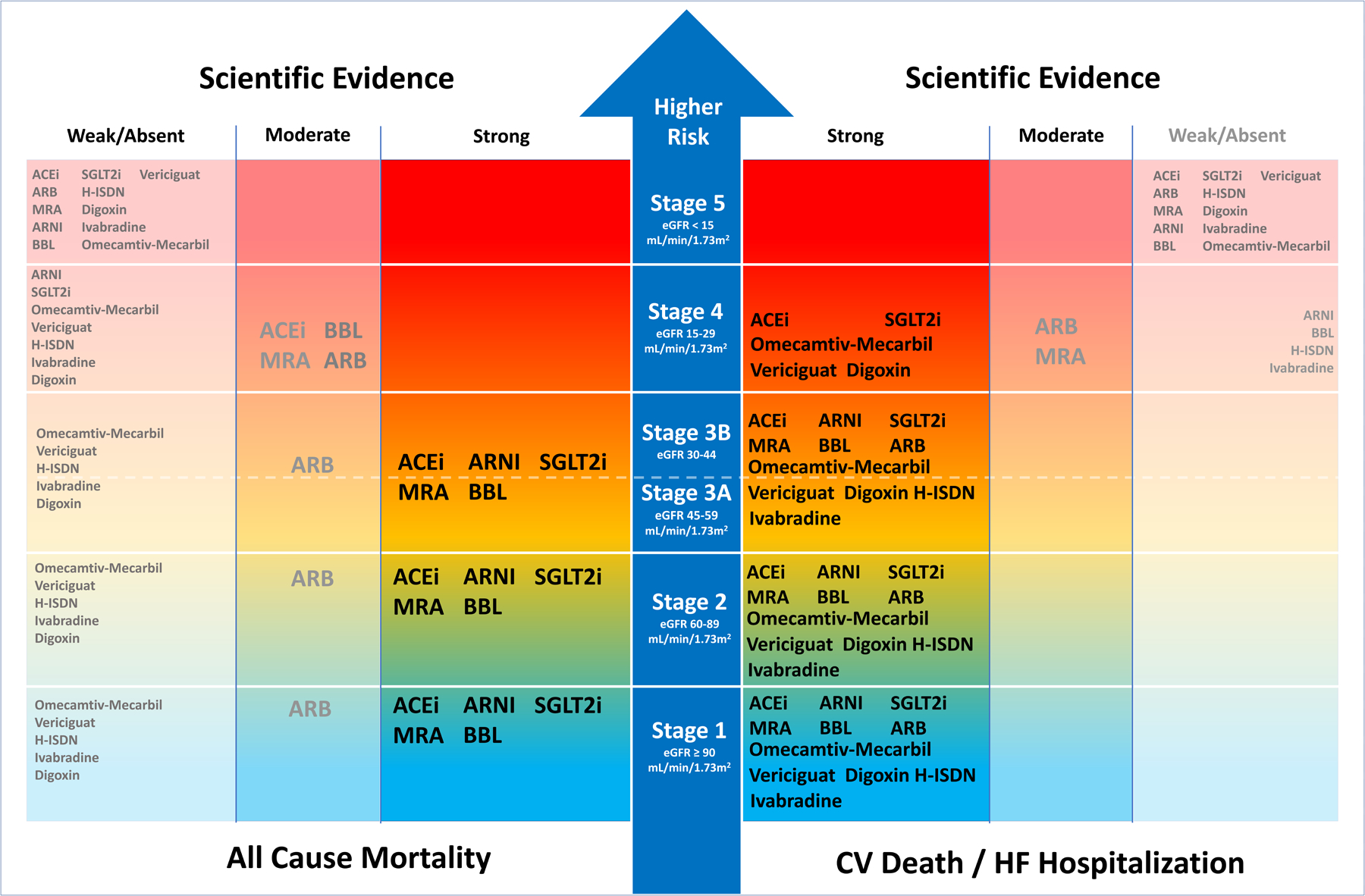
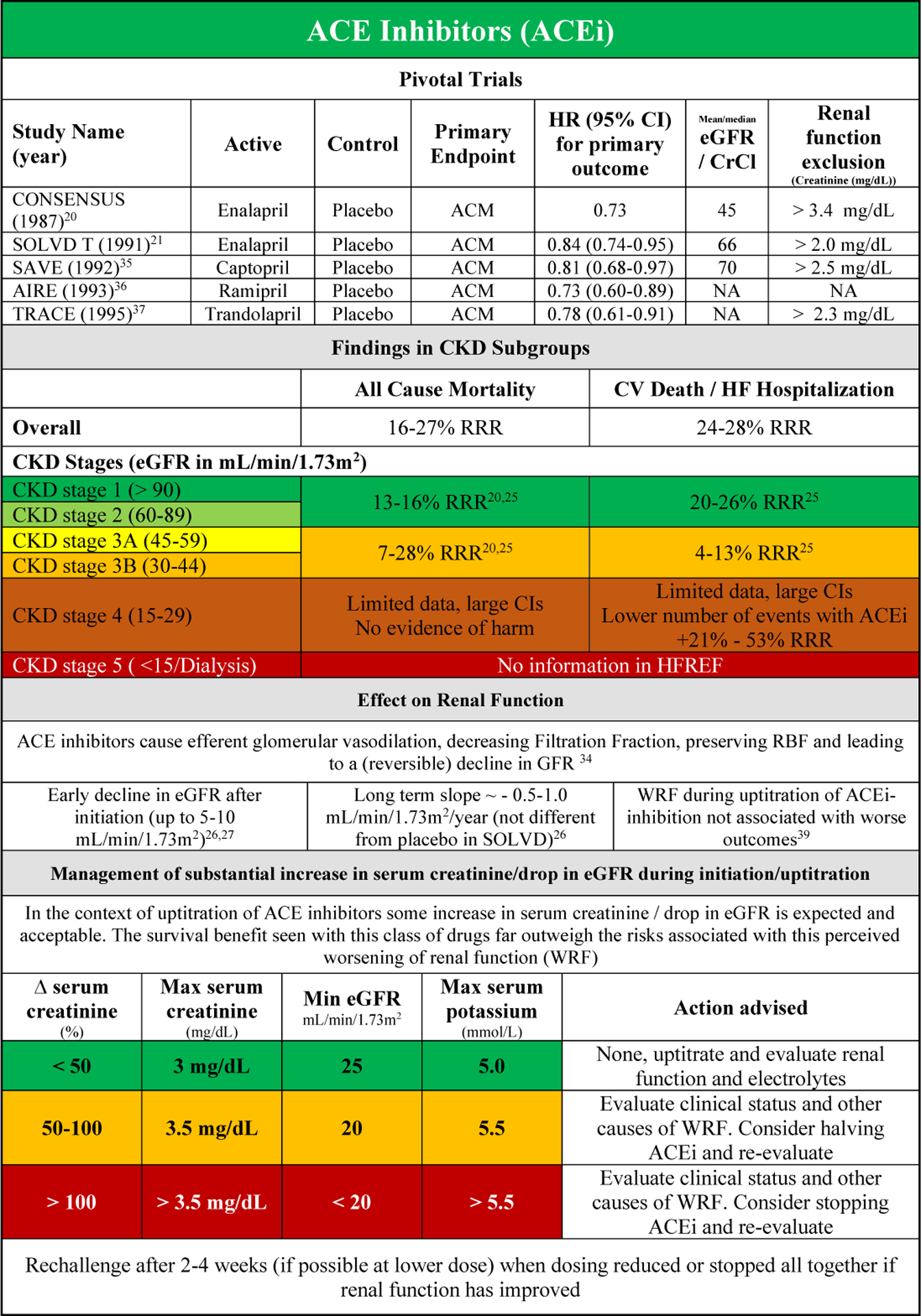
Chronic kidney disease (CKD) as identified by a reduced estimated glomerular filtration rate (eGFR) is a common comorbidity in patients with heart failure with reduced ejection fraction (HFrEF). The presence of CKD is associated with more severe heart failure, and CKD itself is a strong independent risk factor of poor cardiovascular outcome. Furthermore, the presence of CKD often influences the decision to start, uptitrate, or discontinue possible life-saving HFrEF therapies. Because pivotal HFrEF randomized clinical trials have historically excluded patients with stage 4 and 5 CKD (eGFR <30 mL/min/1.73 m), information on the efficacy and tolerability of HFrEF therapies in these patients is limited. However, more recent HFrEF trials with novel classes of drugs included patients with more severe CKD. In this review on medical therapy in patients with HFrEF and CKD, we show that for both all-cause mortality and the combined end point of cardiovascular death or heart failure hospitalization, most drug classes are safe and effective up to CKD stage 3B (eGFR minimum 30 mL/min/1.73 m). For more severe CKD (stage 4), there is evidence of safety and efficacy of sodium glucose cotransporter 2 inhibitors, and to a lesser extent, angiotensin-converting enzyme inhibitors, vericiguat, digoxin and omecamtiv mecarbil, although this evidence is restricted to improvement of cardiovascular death/heart failure hospitalization. Data are lacking on the safety and efficacy for any HFrEF therapies in CKD stage 5 (eGFR < 15 mL/min/1.73 m or dialysis) for either end point. Last, although an initial decline in eGFR is observed on initiation of several HFrEF drug classes (angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers/mineralocorticoid receptor antagonists/angiotensin receptor blocker neprilysin inhibitors/sodium glucose cotransporter 2 inhibitors), renal function often stabilizes over time, and the drugs maintain their clinical efficacy. A decline in eGFR in the context of a stable or improving clinical condition should therefore not be cause for concern and should not lead to discontinuation of life-saving HFrEF therapies.
慢性肾脏病(CKD)是射血分数降低的心力衰竭(HFrEF)患者常见的合并症,其特征是肾小球滤过率(eGFR)降低。CKD 的存在与更严重的心衰相关,而且 CKD 本身是心血管不良结局的一个强有力的独立危险因素。此外,CKD 的存在往往影响开始、调整剂量或停止可能挽救生命的 HFrEF 治疗的决策。由于历史上关键的 HFrEF 随机临床试验排除了 4 期和 5 期 CKD(eGFR <30 mL/min/1.73 m)患者,因此关于这些患者 HFrEF 治疗的疗效和耐受性的信息有限。然而,最近的 HFrEF 试验纳入了更严重 CKD 的新型药物类别患者。在这篇关于 HFrEF 和 CKD 患者药物治疗的综述中,我们表明,对于全因死亡率和心血管死亡或心力衰竭住院的联合终点,大多数药物类别在 CKD 3B 期(eGFR 最小值为 30 mL/min/1.73 m)内是安全有效的。对于更严重的 CKD(4 期),有钠-葡萄糖共转运蛋白 2 抑制剂安全有效的证据,在较小程度上,血管紧张素转换酶抑制剂、维立西呱、地高辛和 omecamtiv mecarbil 也有安全有效的证据,但这些证据仅限于改善心血管死亡/心力衰竭住院。对于任何 HFrEF 治疗,在 CKD 5 期(eGFR <15 mL/min/1.73 m 或透析),均缺乏用于这两个终点的安全性和疗效数据。最后,尽管几种 HFrEF 药物类别(血管紧张素转换酶抑制剂/血管紧张素 II 受体阻滞剂/盐皮质激素受体拮抗剂/血管紧张素受体阻滞剂脑啡肽酶抑制剂/钠-葡萄糖共转运蛋白 2 抑制剂)起始时 eGFR 会出现初始下降,但肾功能通常会随时间稳定,而且这些药物保持其临床疗效。因此,在临床状况稳定或改善的情况下 eGFR 下降不应引起关注,也不应导致停止挽救生命的 HFrEF 治疗。