Brumme Zabrina L, Mwimanzi Francis, Lapointe Hope R, Cheung Peter K, Sang Yurou, Duncan Maggie C, Yaseen Fatima, Agafitei Olga, Ennis Siobhan, Ng Kurtis, Basra Simran, Lim Li Yi, Kalikawe Rebecca, Speckmaier Sarah, Moran-Garcia Nadia, Young Landon, Ali Hesham, Ganase Bruce, Umviligihozo Gisele, Omondi F Harrison, Atkinson Kieran, Sudderuddin Hanwei, Toy Junine, Sereda Paul, Burns Laura, Costiniuk Cecilia T, Cooper Curtis, Anis Aslam H, Leung Victor, Holmes Daniel, DeMarco Mari L, Simons Janet, Hedgcock Malcolm, Romney Marc G, Barrios Rolando, Guillemi Silvia, Brumme Chanson J, Pantophlet Ralph, Montaner Julio S G, Niikura Masahiro, Harris Marianne, Hull Mark, Brockman Mark A
Faculty of Health Sciences, Simon Fraser University, Burnaby, Canada.
British Columbia Centre for Excellence in HIV/AIDS, Vancouver, Canada.
NPJ Vaccines. 2022 Feb 28;7(1):28. doi: 10.1038/s41541-022-00452-6.
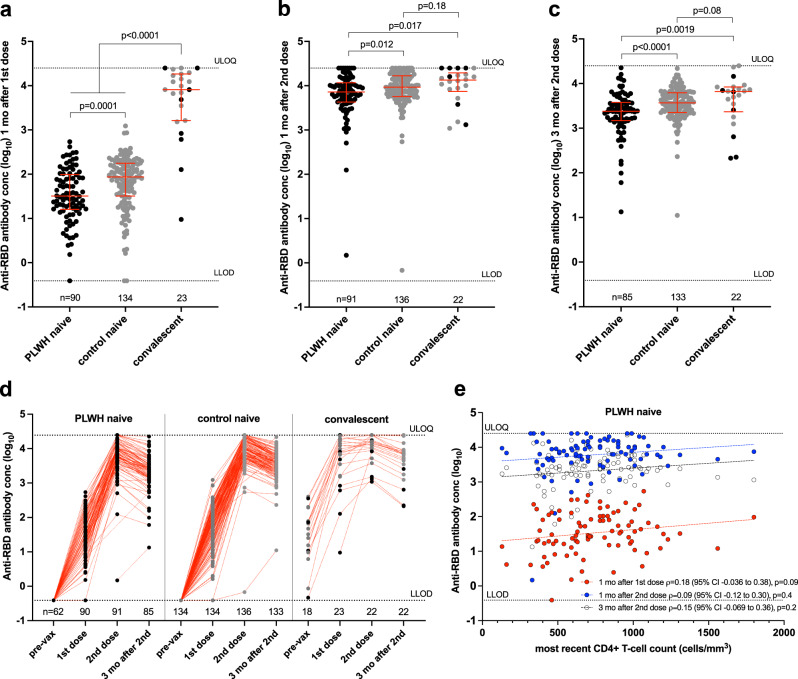
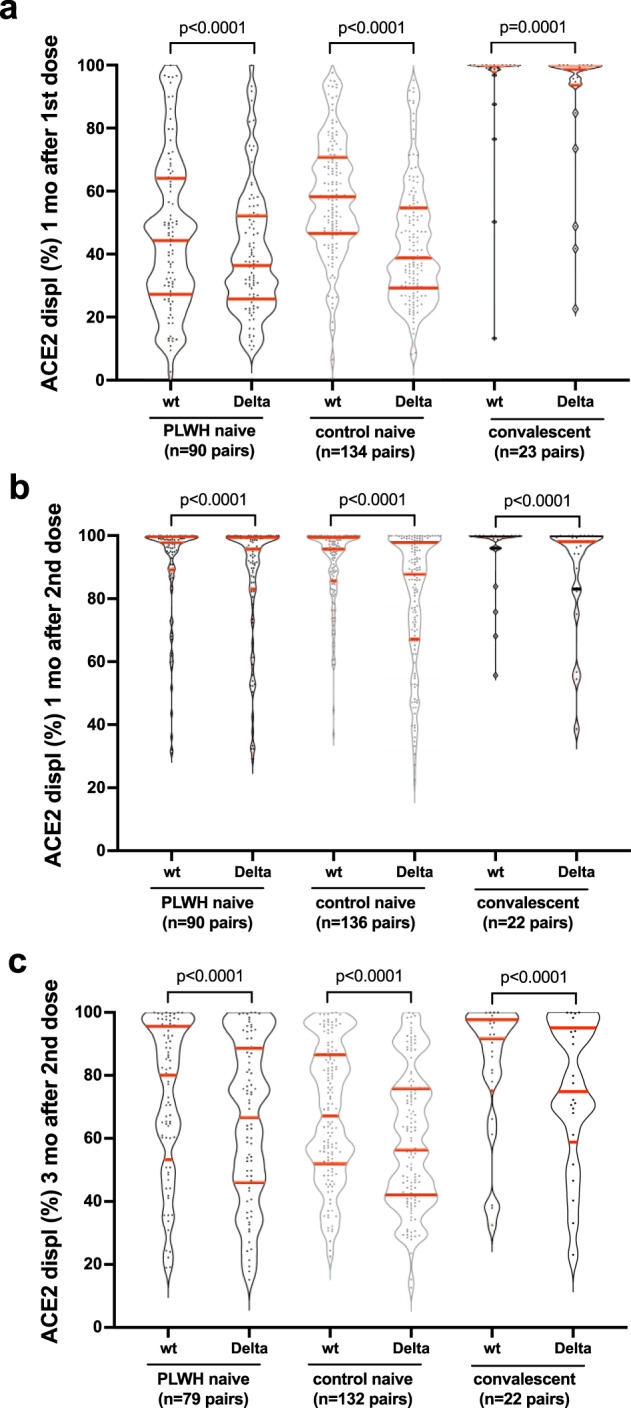
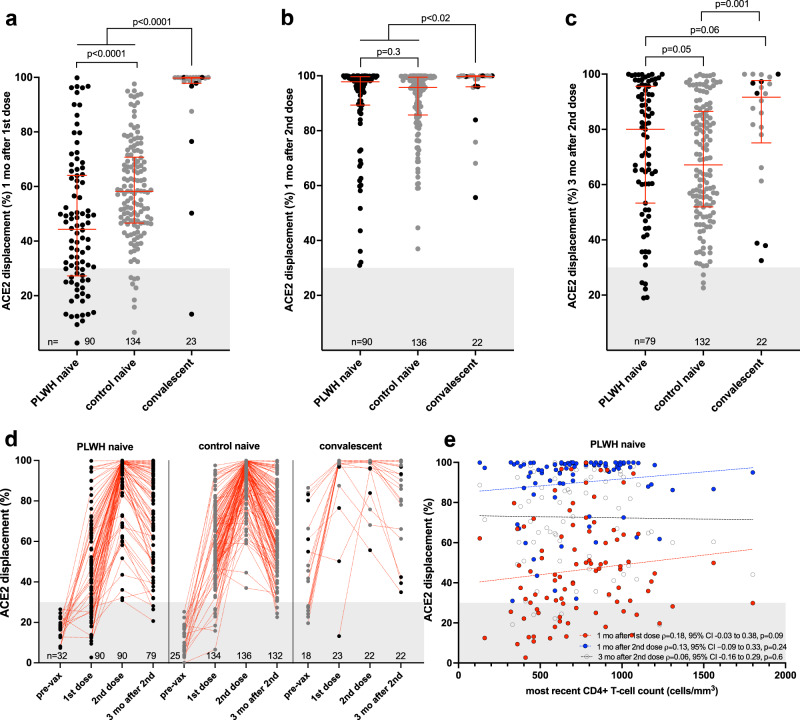
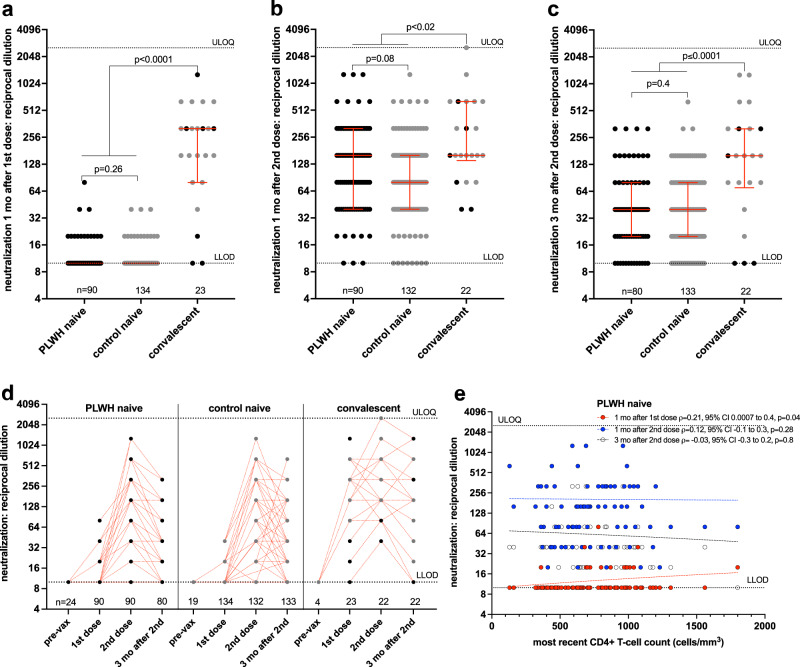
Humoral responses to COVID-19 vaccines in people living with HIV (PLWH) remain incompletely characterized. We measured circulating antibodies against the SARS-CoV-2 spike protein receptor-binding domain (RBD), ACE2 displacement and viral neutralization activities one month following the first and second COVID-19 vaccine doses, and again 3 months following the second dose, in 100 adult PLWH and 152 controls. All PLWH were receiving suppressive antiretroviral therapy, with median CD4+ T-cell counts of 710 (IQR 525-935) cells/mm, though nadir CD4+ T-cell counts ranged as low as <10 cells/mm. After adjustment for sociodemographic, health and vaccine-related variables, HIV infection was associated with lower anti-RBD antibody concentrations and ACE2 displacement activity after one vaccine dose. Following two doses however, HIV was not significantly associated with the magnitude of any humoral response after multivariable adjustment. Rather, older age, a higher burden of chronic health conditions, and dual ChAdOx1 vaccination were associated with lower responses after two vaccine doses. No significant correlation was observed between recent or nadir CD4+ T-cell counts and responses to two vaccine doses in PLWH. These results indicate that PLWH with well-controlled viral loads and CD4+ T-cell counts in a healthy range generally mount strong initial humoral responses to dual COVID-19 vaccination. Factors including age, co-morbidities, vaccine brand, response durability and the rise of new SARS-CoV-2 variants will influence when PLWH will benefit from additional doses. Further studies of PLWH who are not receiving antiretroviral treatment or who have low CD4+ T-cell counts are needed, as are longer-term assessments of response durability.
对感染艾滋病毒者(PLWH)接种新冠病毒疫苗后的体液免疫反应仍未得到充分描述。我们在100名成年PLWH和152名对照者中,测量了在接种第一剂和第二剂新冠病毒疫苗后1个月以及第二剂疫苗后3个月时,针对严重急性呼吸综合征冠状病毒2(SARS-CoV-2)刺突蛋白受体结合域(RBD)的循环抗体、ACE2置换和病毒中和活性。所有PLWH均接受抑制性抗逆转录病毒治疗,CD4 + T细胞计数中位数为710(四分位间距525 - 935)个细胞/mm³,尽管CD4 + T细胞计数最低点低至<10个细胞/mm³。在对社会人口统计学、健康和疫苗相关变量进行调整后,感染艾滋病毒与接种一剂疫苗后较低的抗RBD抗体浓度和ACE2置换活性相关。然而,在接种两剂疫苗后,经过多变量调整,艾滋病毒感染与任何体液免疫反应的强度均无显著关联。相反,年龄较大、慢性健康问题负担较重以及接种两剂ChAdOx1疫苗与接种两剂疫苗后的免疫反应较低有关。在PLWH中,未观察到近期或最低点CD4 + T细胞计数与对两剂疫苗的反应之间存在显著相关性。这些结果表明,病毒载量得到良好控制且CD4 + T细胞计数处于健康范围的PLWH通常对两剂新冠病毒疫苗接种产生强烈的初始体液免疫反应。包括年龄、合并症、疫苗品牌、反应持久性以及新的SARS-CoV-2变体出现等因素,将影响PLWH何时能从额外剂量的疫苗接种中获益。需要对未接受抗逆转录病毒治疗或CD4 + T细胞计数较低的PLWH进行进一步研究,以及对反应持久性进行长期评估。