Texas Tech University Health Sciences Center El Paso TX.
Duke Clinical Res Inst Durham Durham NC.
J Am Heart Assoc. 2022 Mar 15;11(6):e023212. doi: 10.1161/JAHA.121.023212. Epub 2022 Mar 1.
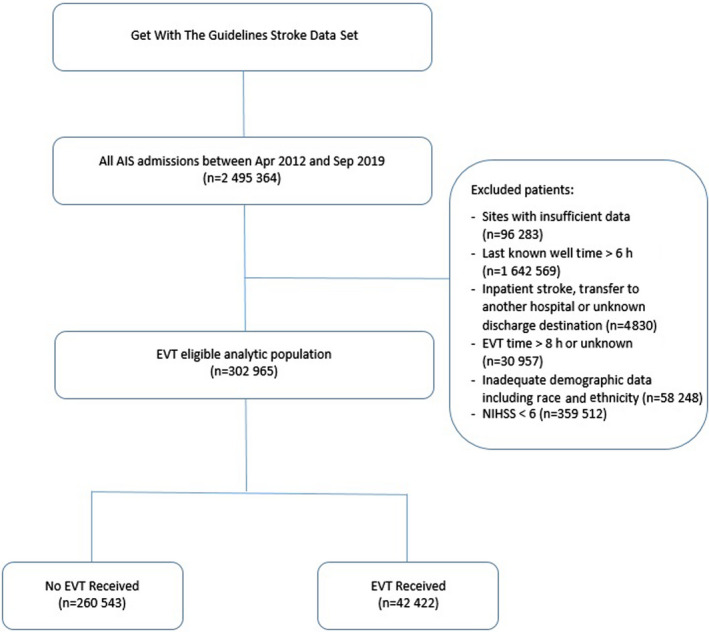
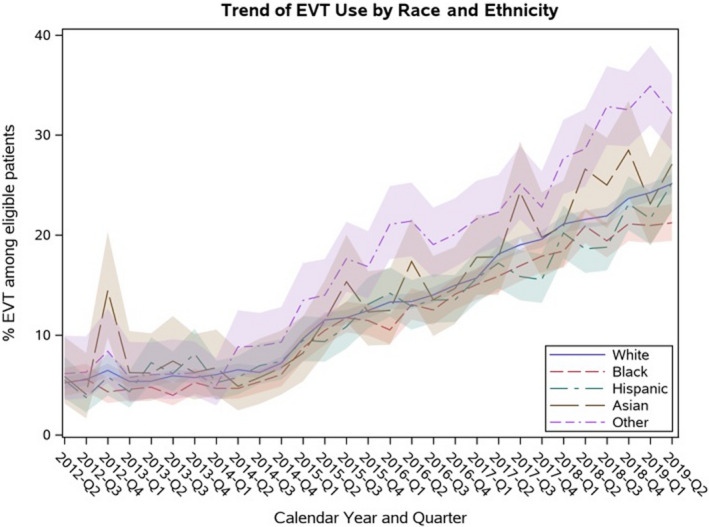
Introduction Endovascular therapy (EVT) use increased following clinical trials publication in 2015, but limited data suggest there may be persistent race and ethnicity differences. Methods and Results We included all patients with acute ischemic stroke arriving within 6 hours of last known well and with National Institute of Health Stroke Scale (NIHSS) score ≥6 between April 2012 and June 2019 in the Get With The Guidelines-Stroke database and evaluated the association between race and ethnicity and EVT use and outcomes, comparing the era before versus after 2015. Of 302 965 potentially eligible patients; 42 422 (14%) underwent EVT. Although EVT use increased over time in all racial and ethnic groups, Black patients had reduced odds of EVT use compared with non-Hispanic White (NHW) patients (adjusted odds ratio [aOR] before 2015, 0.68 [0.58‒0.78]; aOR after 2015, 0.83 [0.76‒0.90]). In-hospital mortality/discharge to hospice was less frequent in Black, Hispanic, and Asian patients compared with NHW. Conversely discharge home was more frequent in Hispanic (29.7%; aOR, 1.28 [1.16‒1.42]), Asian (28.2%; aOR, 1.23 [1.05‒1.44]), and Black (29.1%; aOR, 1.08 [1.00‒1.18]) patients compared with NHW (24%). However, at 3 months, functional independence (modified Rankin Scale, 0-2) occurred less frequently in Black (37.5%; aOR, 0.84 [0.75‒0.95]) and Asian (33%; aOR, 0.79 [0.65‒0.98]) patients compared with NHW patients (38.1%). Conclusions In a large cohort of patients treated with EVT, Black versus NHW patient disparities in EVT use have narrowed over time but still exist. Discharge related outcomes were slightly more favorable in racial and ethnic underrepresented groups; 3-month functional outcomes were worse but improved across all groups with time.
介绍
血管内治疗(EVT)的使用在 2015 年临床试验发表后有所增加,但有限的数据表明,可能仍然存在种族和民族差异。
方法和结果
我们纳入了 2012 年 4 月至 2019 年 6 月期间,在 Get With The Guidelines-Stroke 数据库中所有在最后一次可识别的正常状态后 6 小时内到达且 NIHSS 评分≥6 的急性缺血性卒中患者,并评估了种族和民族与 EVT 使用和结局之间的关联,比较了 2015 年前后的时代差异。在 302965 名可能符合条件的患者中;42422 名(14%)接受了 EVT。尽管所有种族和民族群体的 EVT 使用都随着时间的推移而增加,但与非西班牙裔白人(NHW)患者相比,黑人患者接受 EVT 的可能性降低(2015 年前的调整比值比 [aOR],0.68 [0.58-0.78];2015 年后的 aOR,0.83 [0.76-0.90])。与 NHW 患者相比,黑人、西班牙裔和亚洲患者的住院死亡率/出院至临终关怀的比例较低。相反,西班牙裔(29.7%;aOR,1.28 [1.16-1.42])、亚洲裔(28.2%;aOR,1.23 [1.05-1.44])和黑人(29.1%;aOR,1.08 [1.00-1.18])患者的出院回家的比例高于 NHW(24%)。然而,在 3 个月时,黑人(37.5%;aOR,0.84 [0.75-0.95])和亚洲裔(33%;aOR,0.79 [0.65-0.98])患者的功能独立性(改良 Rankin 量表,0-2)较 NHW 患者(38.1%)发生的频率较低。
结论
在接受 EVT 治疗的大量患者中,黑人与 NHW 患者在 EVT 使用方面的差异随着时间的推移而缩小,但仍存在差异。在代表性不足的种族和民族群体中,与出院相关的结局略为有利;但所有群体的 3 个月功能结局较差,但随着时间的推移都有所改善。