Cheng Yi-Bang, Thijs Lutgarde, Aparicio Lucas S, Huang Qi-Fang, Wei Fang-Fei, Yu Yu-Ling, Barochiner Jessica, Sheng Chang-Sheng, Yang Wen-Yi, Niiranen Teemu J, Boggia José, Zhang Zhen-Yu, Stolarz-Skrzypek Katarzyna, Gilis-Malinowska Natasza, Tikhonoff Valérie, Wojciechowska Wiktoria, Casiglia Edoardo, Narkiewicz Krzysztof, Filipovský Jan, Kawecka-Jaszcz Kalina, Wang Ji-Guang, Li Yan, Staessen Jan A
Department of Cardiovascular Medicine, Shanghai Key Laboratory of Hypertension, Shanghai Institute of Hypertension, State Key Laboratory of Medical Genomics, National Research Centre for Translational Medicine, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, China (Y.-B.C., Q.-F.H., C.-S.S., J.-G.W., Y.L.).
Research Unit Hypertension and Cardiovascular Epidemiology, KU Leuven Department of Cardiovascular Sciences, University of Leuven, Belgium (L.T., F.-F.W., Y.-L.Y., W.-Y.Y., Z.-Y.Z.).
Hypertension. 2022 May;79(5):1101-1111. doi: 10.1161/HYPERTENSIONAHA.121.18773. Epub 2022 Mar 4.
Whether cardiovascular risk is more tightly associated with central (cSBP) than brachial (bSBP) systolic pressure remains debated, because of their close correlation and uncertain thresholds to differentiate cSBP into normotension versus hypertension.
In a person-level meta-analysis of the International Database of Central Arterial Properties for Risk Stratification (n=5576; 54.1% women; mean age 54.2 years), outcome-driven thresholds for cSBP were determined and whether the cross-classification of cSBP and bSBP improved risk stratification was explored. cSBP was tonometrically estimated from the radial pulse wave using SphygmoCor software.
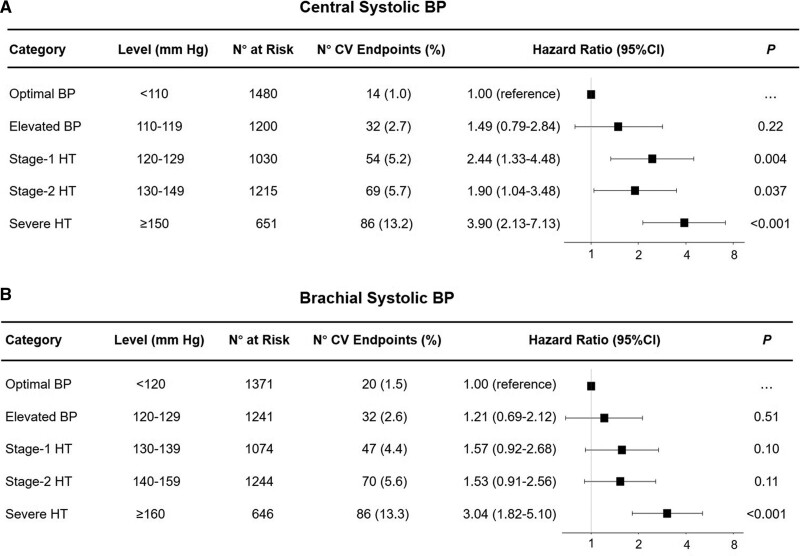
Over 4.1 years (median), 255 composite cardiovascular end points occurred. In multivariable bootstrapped analyses, cSBP thresholds (in mm Hg) of 110.5 (95% CI, 109.1-111.8), 120.2 (119.4-121.0), 130.0 (129.6-130.3), and 149.5 (148.4-150.5) generated 5-year cardiovascular risks equivalent to the American College of Cardiology/American Heart Association bSBP thresholds of 120, 130, 140, and 160. Applying 120/130 mm Hg as cSBP/bSBP thresholds delineated concordant central and brachial normotension (43.1%) and hypertension (48.2%) versus isolated brachial hypertension (5.0%) and isolated central hypertension (3.7%). With concordant normotension as reference, the multivariable hazard ratios for the cardiovascular end point were 1.30 (95% CI, 0.58-2.94) for isolated brachial hypertension, 2.28 (1.21-4.30) for isolated central hypertension, and 2.02 (1.41-2.91) for concordant hypertension. The increased cardiovascular risk associated with isolated central and concordant hypertension was paralleled by cerebrovascular end points with hazard ratios of 3.71 (1.37-10.06) and 2.60 (1.35-5.00), respectively.
Irrespective of the brachial blood pressure status, central hypertension increased cardiovascular and cerebrovascular risk indicating the importance of controlling central hypertension.
由于中心收缩压(cSBP)与肱动脉收缩压(bSBP)密切相关,且区分cSBP正常血压与高血压的阈值尚不确定,因此心血管风险与cSBP的关联是否比bSBP更紧密仍存在争议。
在一项针对国际中心动脉特性风险分层数据库(n = 5576;54.1%为女性;平均年龄54.2岁)的个体水平荟萃分析中,确定了cSBP的预后驱动阈值,并探讨了cSBP和bSBP的交叉分类是否能改善风险分层。使用SphygmoCor软件通过桡动脉脉搏波以眼压测量法估算cSBP。
在4.1年(中位数)期间,发生了255个复合心血管终点事件。在多变量自抽样分析中,cSBP阈值(以毫米汞柱为单位)为110.5(95%置信区间,109.1 - 111.8)、120.2(119.4 - 121.0)、130.0(129.6 - 130.3)和149.5(148.4 - 150.5)时产生的5年心血管风险与美国心脏病学会/美国心脏协会bSBP阈值为 120、130、140和160时相当。将120/130毫米汞柱作为cSBP/bSBP阈值可区分出一致的中心和肱动脉正常血压(43.1%)、高血压(48.2%),孤立性肱动脉高血压(5.0%)和孤立性中心高血压(3.7%)。以一致的正常血压为参照,孤立性肱动脉高血压的心血管终点多变量风险比为1.30(95%置信区间,0.58 - 2.94),孤立性中心高血压为2.28(1.21 - 4.30),一致性高血压为2.02(1.41 - 2.91)。与孤立性中心高血压和一致性高血压相关的心血管风险增加与脑血管终点事件平行,风险比分别为3.71(1.37 - 10.06)和2.60(1.35 - 5.00)。
无论肱动脉血压状况如何,中心高血压都会增加心血管和脑血管风险,这表明控制中心高血压的重要性。