Gupta Varun, Noh Ka-Won, Maschek Hansjörg, Thal Stefan, Welter Stefan
Department of Thoracic Surgery, Lung Clinic Hemer, Theo-Funccius Str. 1, 58675, Hemer, Germany.
Institute of Pathology, University Hospital Cologne, Kerpener Str. 62, 50937, Cologne, Germany.
Respir Med Case Rep. 2022 Feb 18;36:101603. doi: 10.1016/j.rmcr.2022.101603. eCollection 2022.
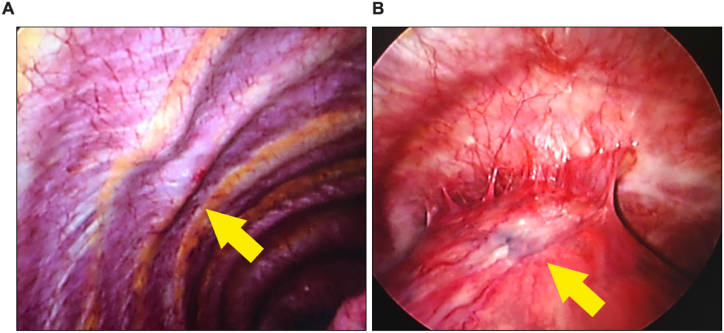
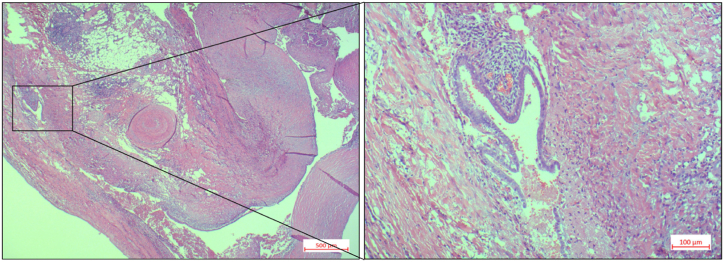
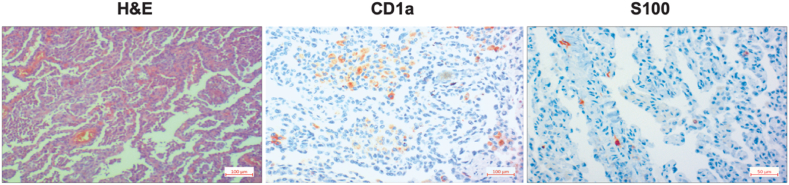
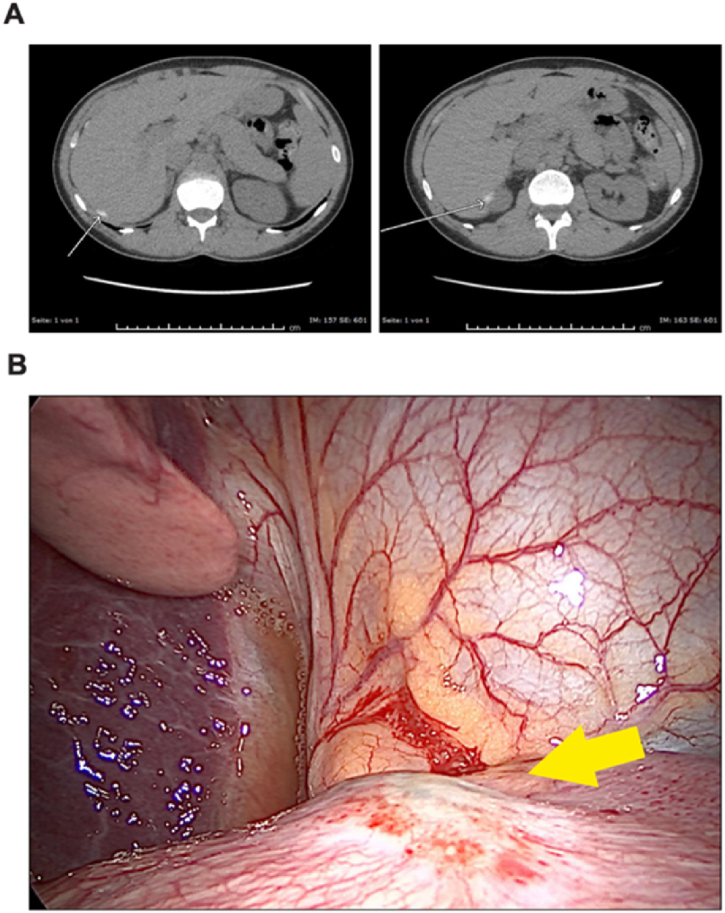
Spontaneous pneumothorax (SP) in women of reproductive age with causes such as thoracic endometriosis syndrome (TES) presents a diagnostic and therapeutic challenge. A 33-year-old women was treated conservatively with chest tube insertion for a first occurrence of a right-sided pneumothorax in September 2015. In January 2016, a right-sided video-assisted thoracoscopic surgery (VATS) wedge resection and partial parietal pleurectomy was performed due to a recurrence. A right-sided VATS was again performed in December 2016 with multiple wedge resections and a total pleurectomy revealing a pulmonary Langerhans' cell histiocytosis (PLCH) in the histological and immunohistochemical examinations. The patient was recommended an abstinence of smoking and further course was unremarkable until May 2019, when due to a recurrent pneumothorax, she received a talc pleurodesis via right-sided VATS. Due to yet another recurrence, she underwent a talc slurry pleurodesis over a right sided chest drain. In March 2020 due to recurrence, a right-sided VATS was performed and a blueish nodular lesion was resected from the diaphragm. The histological examination revealed an endometriosis with a diagnosis of TES. Since the patient did not exhibit a temporal relationship between her periods and the onset of pneumothorax symptoms, a final diagnosis of non-catamenial endometriosis-related pneumothorax was made. The patient is currently continuing smoking abstinence and is under hormone therapy. She has not presented with a recurrence. In clinical practice, it is important not to just relay on the information available to us, but to reevaluate the patient history to uncover new clues leading to a new diagnosis.
患有诸如胸膜子宫内膜异位症综合征(TES)等病因的育龄期女性自发性气胸(SP),在诊断和治疗上具有挑战性。一名33岁女性于2015年9月首次发生右侧气胸时,接受了胸腔闭式引流保守治疗。2016年1月,因复发进行了右侧电视辅助胸腔镜手术(VATS)楔形切除术和部分壁层胸膜切除术。2016年12月再次进行右侧VATS,进行了多次楔形切除术和全胸膜切除术,组织学和免疫组化检查显示为肺朗格汉斯细胞组织细胞增多症(PLCH)。建议患者戒烟,直至2019年5月病情平稳,当时因气胸复发,她通过右侧VATS接受了滑石粉胸膜固定术。由于再次复发,她通过右侧胸腔引流管接受了滑石粉悬液胸膜固定术。2020年3月因复发,进行了右侧VATS,并从膈肌切除了一个蓝色结节性病变。组织学检查显示为子宫内膜异位症,诊断为TES。由于患者月经周期与气胸症状发作之间未表现出时间关系,最终诊断为非月经期子宫内膜异位症相关性气胸。该患者目前继续戒烟并接受激素治疗。她未再复发。在临床实践中,重要的是不要仅仅依赖我们所掌握的信息,而是要重新评估患者病史以发现导致新诊断的新线索。