Department of Global HIV, Hepatitis and Sexually Transmitted Infections Programmes, WHO, Geneva, Switzerland; Centre for Infectious Disease Epidemiology and Research, School of Public Health and Family Medicine, University of Cape Town, Cape Town, South Africa.
Centre for Infectious Disease Epidemiology and Research, School of Public Health and Family Medicine, University of Cape Town, Cape Town, South Africa.
Lancet HIV. 2022 Mar;9(3):e150-e159. doi: 10.1016/S2352-3018(21)00329-5.
The identification and appropriate management of people with advanced HIV disease is a key component in the HIV response. People with HIV who are hospitalised are at a higher risk of death, a risk that might persist after discharge. The aims of this study were to estimate the frequency of negative post-discharge outcomes, and to determine risk factors for such outcomes in people with HIV.
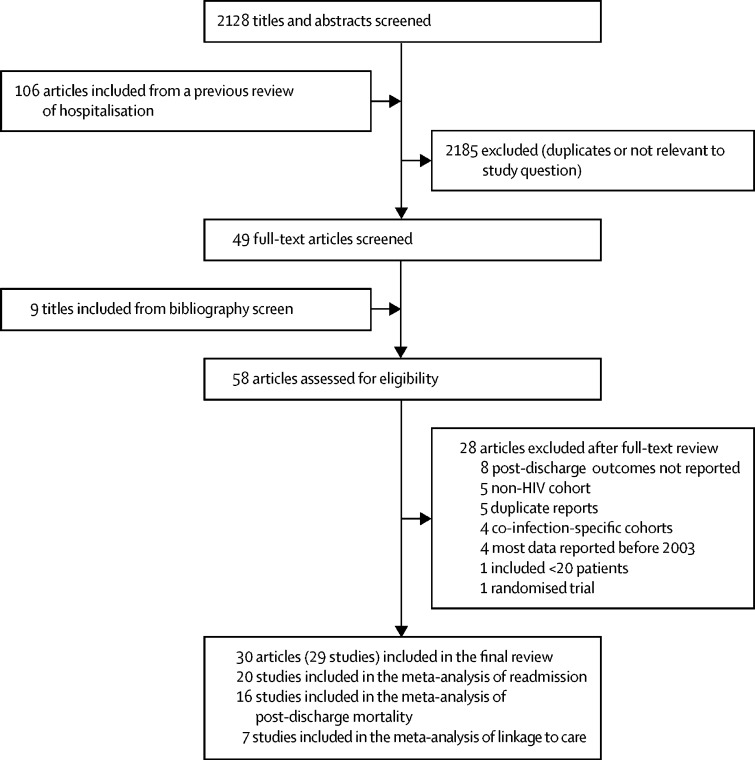
Using a broad search strategy combining terms for hospital discharge and HIV infection, we searched MEDLINE via PubMed and Embase from Jan 1, 2003 to Nov 30, 2021 to identify studies reporting outcomes among people with HIV following discharge from hospital. We estimated pooled proportions of readmissions and deaths after hospital discharge using random-effects models. We also did subgroup analyses by setting, region, duration of follow-up, and advanced HIV status at admission, and sensitivity analyses to assess heterogeneity.
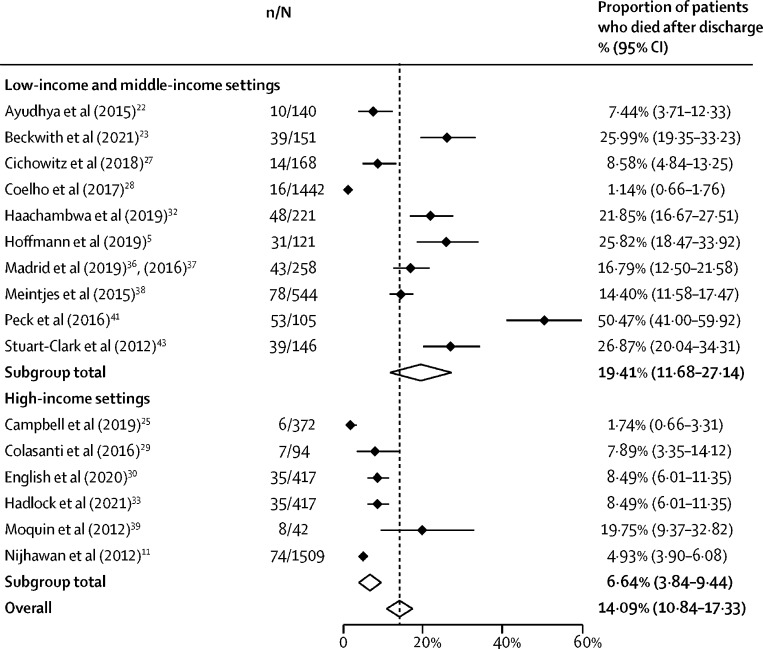
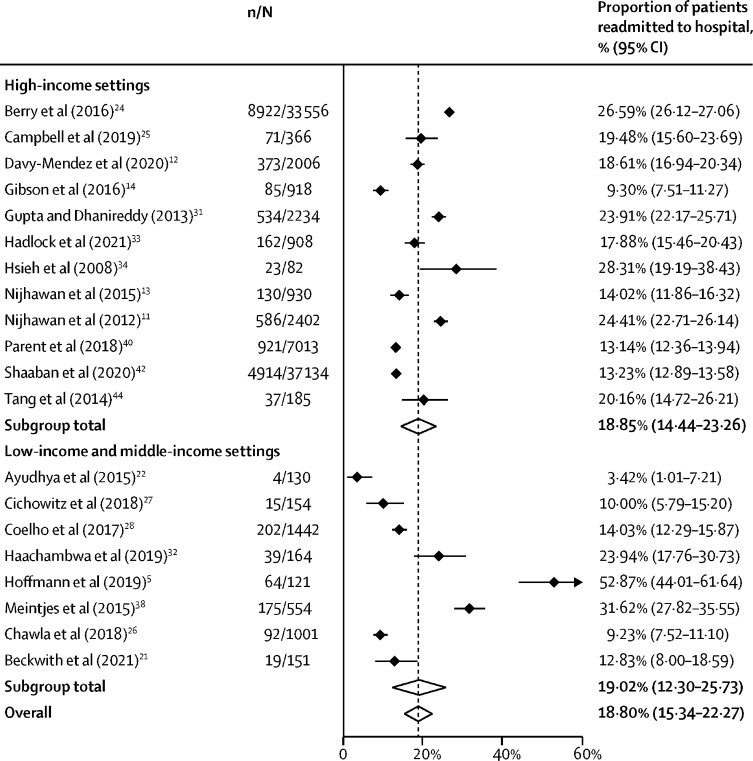
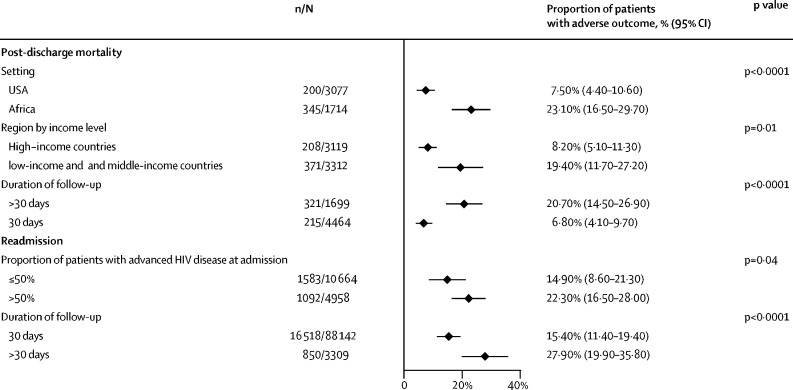
We obtained data from 29 cohorts, which reported outcomes of people living with HIV after hospital discharge in 92 781 patients. The pooled proportion of patients readmitted to hospital after discharge was 18·8% (95% CI 15·3-22·3) and 14·1% (10·8-17·3) died post-discharge. In sensitivity analyses, no differences were identified in the proportion of patients who were readmitted or died when comparing studies published before 2016 with those published after 2016. Post-discharge mortality was higher in studies from Africa (23·1% [16·5-29·7]) compared with the USA (7·5% [4·4-10·6]). For studies that reported both post-discharge mortality and readmission, the pooled proportion of patients who had this composite adverse outcome was 31·7% (23·9-39·5). Heterogeneity was moderate, and largely explained by patient status and linkage to care. Reported risk factors for readmission included low CD4 cell count at admission, longer length of stay, discharge against medical advice, and not linking to care following discharge; inpatient treatment with antiretroviral therapy (ART) during hospitalisation was protective of post-discharge mortality.
More than a quarter of patients with HIV had an adverse outcome after hospital discharge with no evidence of improvement in the past 15 years. This systematic review highlights the importance of ensuring post-discharge referral and appropriate management, including ART, to reduce mortality and readmission to hospital among this group of high-risk patients.
Bill & Melinda Gates Foundation.
For the French and Spanish translations of the abstract see Supplementary Materials section.
识别和适当管理晚期 HIV 疾病患者是 HIV 应对工作的关键组成部分。住院的 HIV 患者死亡风险更高,这种风险在出院后可能仍然存在。本研究的目的是评估 HIV 患者出院后负面结局的频率,并确定此类结局的危险因素。
我们使用广泛的搜索策略,结合出院和 HIV 感染的术语,通过 PubMed 中的 MEDLINE 和 Embase 从 2003 年 1 月 1 日至 2021 年 11 月 30 日进行检索,以确定报告出院后 HIV 患者结局的研究。我们使用随机效应模型估计出院后再入院和死亡的汇总比例。我们还按设置、地区、随访时间和入院时的晚期 HIV 状况进行了亚组分析,并进行敏感性分析以评估异质性。
我们从 29 项队列研究中获取了数据,这些研究报告了 92781 名 HIV 感染者出院后的结局。出院后再入院的患者比例为 18.8%(95%CI 15.3-22.3),出院后死亡的比例为 14.1%(10.8-17.3)。在敏感性分析中,比较 2016 年前发表的研究和 2016 年后发表的研究,未发现患者再入院或死亡的比例存在差异。与美国(4.4%-10.6%)相比,来自非洲的研究(23.1%[16.5-29.7])中出院后的死亡率更高。对于同时报告出院后死亡率和再入院率的研究,该复合不良结局患者的比例为 31.7%(23.9-39.5)。异质性中等,主要由患者状况和与护理的联系解释。再入院的报告危险因素包括入院时 CD4 细胞计数低、住院时间长、未经医嘱出院和出院后未与护理机构联系;住院期间接受抗逆转录病毒治疗(ART)可降低出院后的死亡率。
超过四分之一的 HIV 患者出院后出现不良结局,在过去 15 年中没有证据表明情况有所改善。本系统评价强调了确保出院后转介和适当管理的重要性,包括 ART,以降低这群高危患者的死亡率和再入院率。
比尔及梅琳达·盖茨基金会。