Department of Orthopaedic Surgery, University of Toyama, Faculty of Medicine, 2630 Sugitani, Toyama, Toyama, 930-0194, Japan.
BMC Musculoskelet Disord. 2022 Mar 4;23(1):208. doi: 10.1186/s12891-022-05158-3.
Severe postsurgical pain in posterior spinal fusion is common. Multimodality analgesia, including opioid-based patient-controlled analgesia (PCA), is commonly used, but opioid-related adverse events such as nausea and vomiting are sometimes a problem. We used a ropivacaine-epinephrine-dexamethasone mixture given as one-time local bilateral submyofascial injections at the operated levels added to conventional multimodality analgesia including PCA for postoperative pain control in one group of patients to confirm whether administration of this mixture reduced postoperative pain and opioid use status post posterior spinal fusion.
We retrospectively reviewed 67 consecutive patients who had undergone posterior fusion surgery for adolescent idiopathic scoliosis (AIS), 35 of whom were treated with conventional analgesia that consisted mainly of PCA (control group) and 32 of whom were treated with one-time submyofascial injections of a ropivacaine-epinephrine-dexamethasone mixture (submyofascial injection group) added to conventional multimodality analgesia. We compared postsurgical pain levels and the amount of opioid use over the first 48 h after surgery, as well as physical activity levels and adverse events 2 weeks after surgery.
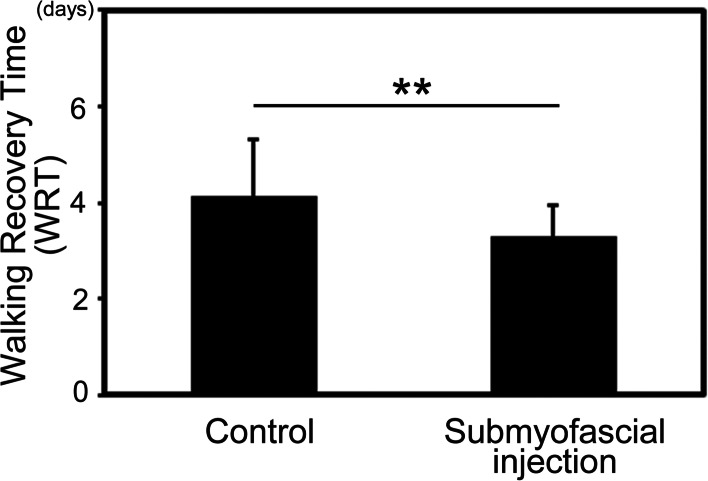
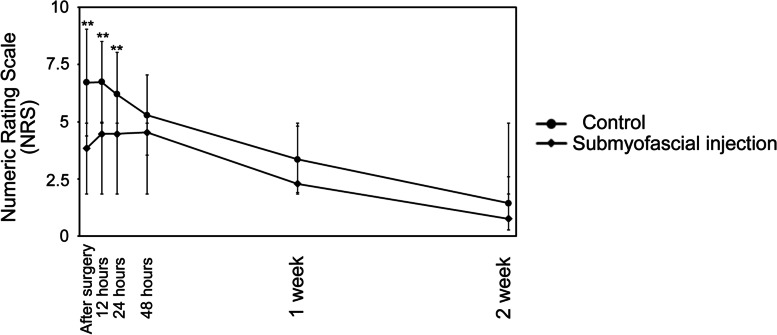
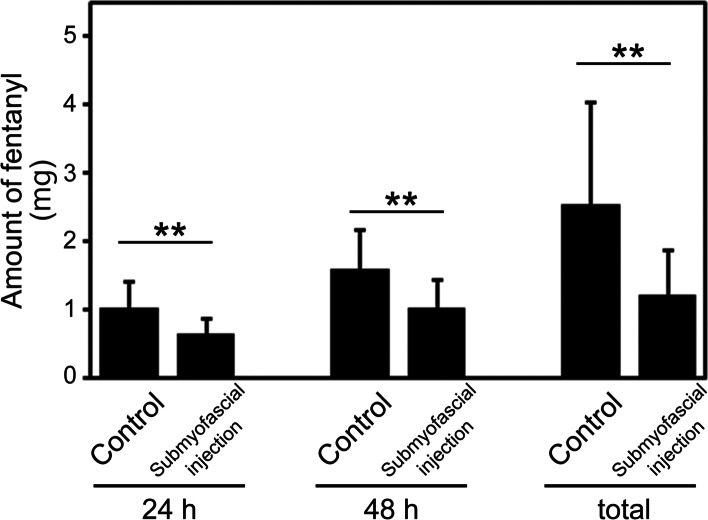
Postsurgical pain quantified by a numeric rating scale (1-10) in the submyofascial injection group was significantly lower than that in the control group. The amount of fentanyl use was significantly less in the submyofascial injection group at 24 h, 48 h, and all subsequent periods after surgery. In addition, Walking Recovery Time (WRT) defined as the number of days until the first event of ambulation was significantly less in the submyofascial injection group (3.3 d vs 4.1 d, P = 0.0007)). Laxative use was significantly less in the submyofascial injection group (0.3 times vs 1.3 times, P = 0.02).
One-time submyofascial injections at the operated levels with a ropivacaine-epinephrine-dexamethasone mixture after spinal fusion surgery reduced pain, opioid consumption, and opioid-related adverse events. This technique can contribute significantly to postoperative analgesia.
脊柱融合术后严重的术后疼痛很常见。多模式镇痛,包括基于阿片类药物的患者自控镇痛(PCA),通常被使用,但阿片类药物相关的不良反应,如恶心和呕吐,有时是一个问题。我们使用罗哌卡因-肾上腺素-地塞米松混合物,在手术水平进行一次性双侧肌筋膜下注射,加入常规多模式镇痛,包括 PCA,用于一组患者的术后疼痛控制,以确认这种混合物的给药是否减少了脊柱融合术后的术后疼痛和阿片类药物使用情况。
我们回顾性分析了 67 例接受青少年特发性脊柱侧凸(AIS)后路融合手术的连续患者,其中 35 例接受了主要为 PCA 的常规镇痛治疗(对照组),32 例接受了罗哌卡因-肾上腺素-地塞米松混合物一次性肌筋膜下注射(肌筋膜下注射组)加常规多模式镇痛治疗。我们比较了术后 48 小时内的术后疼痛水平和阿片类药物的使用量,以及术后 2 周的身体活动水平和不良反应。
肌筋膜下注射组的数字评分量表(1-10)量化的术后疼痛明显低于对照组。在术后 24 小时、48 小时和所有后续时间段,肌筋膜下注射组芬太尼的使用量明显减少。此外,定义为首次行走的天数的行走恢复时间(WRT)在肌筋膜下注射组明显减少(3.3 d 与 4.1 d,P = 0.0007)。肌筋膜下注射组的通便剂使用量明显减少(0.3 次与 1.3 次,P = 0.02)。
脊柱融合术后在手术水平进行一次性肌筋膜下罗哌卡因-肾上腺素-地塞米松混合物注射,可减轻疼痛、阿片类药物的消耗和阿片类药物相关的不良反应。这种技术可以显著促进术后镇痛。