National Heart and Lung InstituteImperial College London London UK.
National Institute for Health Research Imperial Biomedical Research CentreImperial College London and Imperial College Healthcare NHS Trust London UK.
J Am Heart Assoc. 2022 Mar 15;11(6):e024260. doi: 10.1161/JAHA.121.024260. Epub 2022 Mar 8.
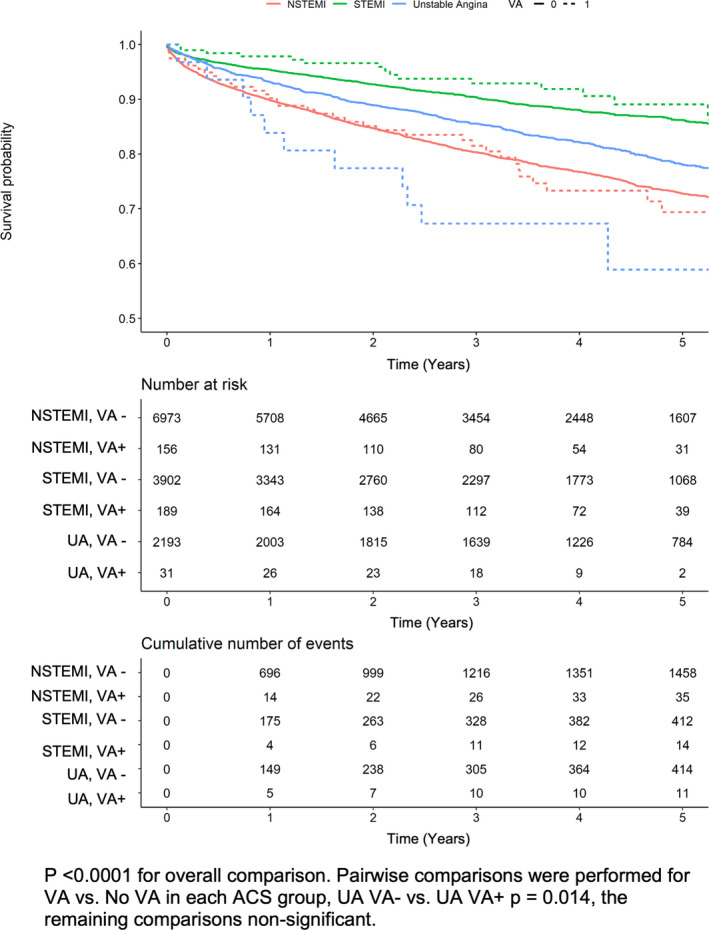
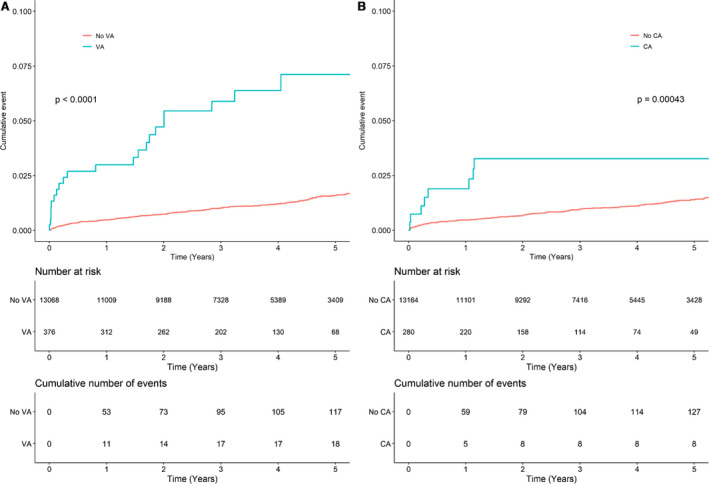
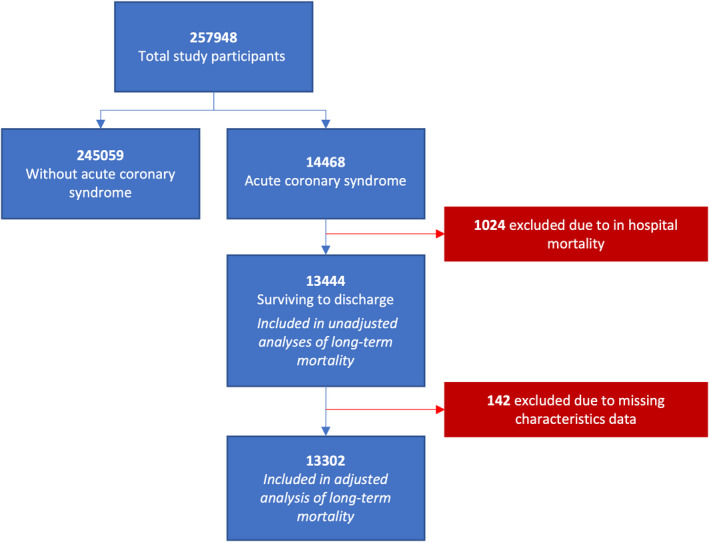
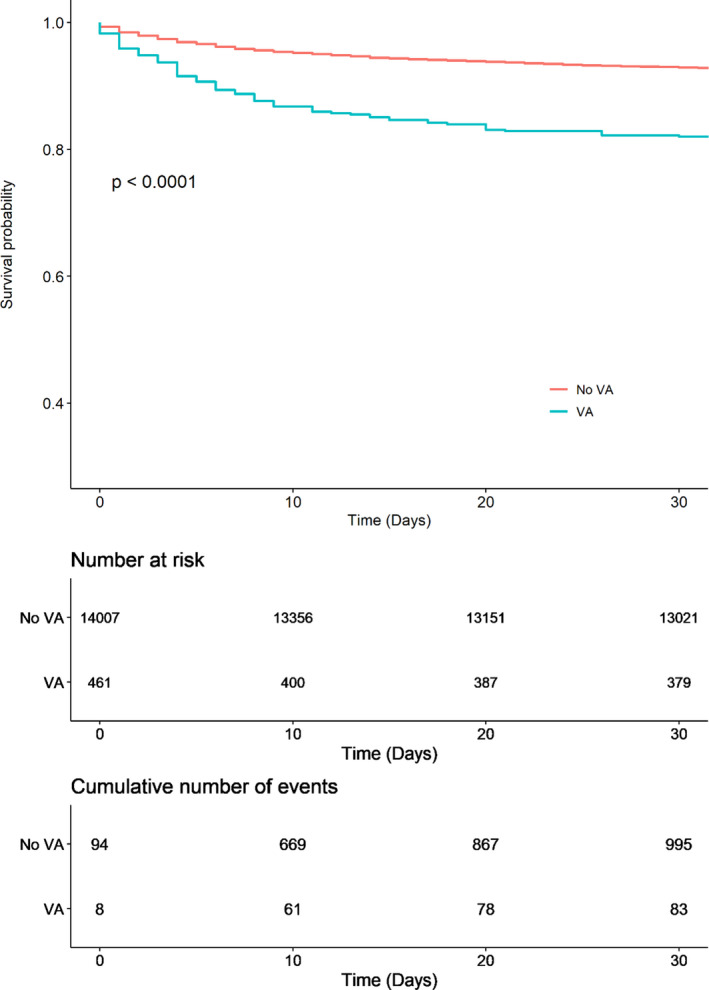
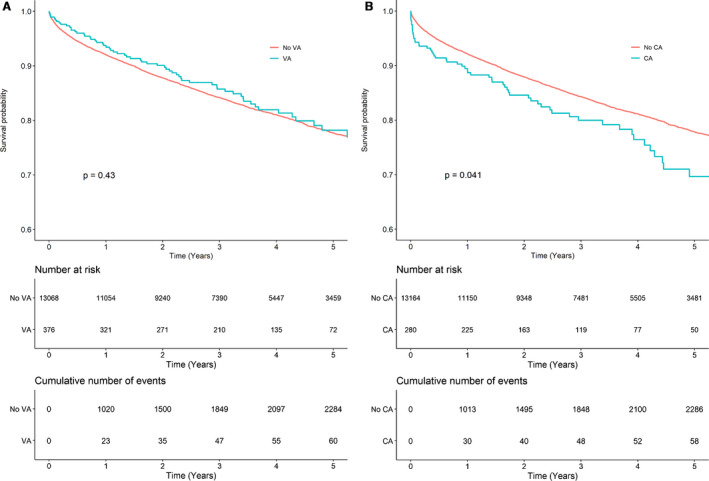
Background A minority of acute coronary syndrome (ACS) cases are associated with ventricular arrhythmias (VA) and/or cardiac arrest (CA). We investigated the effect of VA/CA at the time of ACS on long-term outcomes. Methods and Results We analyzed routine clinical data from 5 National Health Service trusts in the United Kingdom, collected between 2010 and 2017 by the National Institute for Health Research Health Informatics Collaborative. A total of 13 444 patients with ACS, 376 (2.8%) of whom had concurrent VA, survived to hospital discharge and were followed up for a median of 3.42 years. Patients with VA or CA at index presentation had significantly increased risks of subsequent VA during follow-up (VA group: adjusted hazard ratio [HR], 4.15 [95% CI, 2.42-7.09]; CA group: adjusted HR, 2.60 [95% CI, 1.23-5.48]). Patients who suffered a CA in the context of ACS and survived to discharge also had a 36% increase in long-term mortality (adjusted HR, 1.36 [95% CI, 1.04-1.78]), although the concurrent diagnosis of VA alone during ACS did not affect all-cause mortality (adjusted HR, 1.03 [95% CI, 0.80-1.33]). Conclusions Patients who develop VA or CA during ACS who survive to discharge have increased risks of subsequent VA, whereas those who have CA during ACS also have an increase in long-term mortality. These individuals may represent a subgroup at greater risk of subsequent arrhythmic events as a result of intrinsically lower thresholds for developing VA.
少数急性冠状动脉综合征(ACS)病例与室性心律失常(VA)和/或心搏骤停(CA)有关。我们研究了 ACS 时 VA/CA 对长期预后的影响。
我们分析了英国 5 家国民保健服务信托机构在 2010 年至 2017 年期间通过国家卫生研究院健康信息学合作收集的常规临床数据。共有 13444 例 ACS 患者,其中 376 例(2.8%)并发 VA,存活至出院并随访中位数为 3.42 年。在指数期出现 VA 或 CA 的患者在随访期间发生后续 VA 的风险显著增加(VA 组:调整后的危险比[HR],4.15[95%CI,2.42-7.09];CA 组:调整后的 HR,2.60[95%CI,1.23-5.48])。在 ACS 中发生 CA 并存活至出院的患者长期死亡率也增加了 36%(调整后的 HR,1.36[95%CI,1.04-1.78]),尽管 ACS 期间并发 VA 单独诊断不会影响全因死亡率(调整后的 HR,1.03[95%CI,0.80-1.33])。
ACS 期间发生 VA 或 CA 并存活至出院的患者发生后续 VA 的风险增加,而 ACS 期间发生 CA 的患者长期死亡率也增加。这些个体可能代表因内在 VA 发生阈值较低而更容易发生心律失常事件的亚组。