Department of Clinical Neurophysiology and MEG Center, Amsterdam Neuroscience, Vrije Universiteit Amsterdam, Amsterdam UMC, Amsterdam, The Netherlands.
Department of Neurosurgery, Amsterdam Neuroscience, Vrije Universiteit Amsterdam, Amsterdam UMC, Amsterdam, The Netherlands.
Sci Rep. 2022 Mar 8;12(1):4086. doi: 10.1038/s41598-022-07730-2.
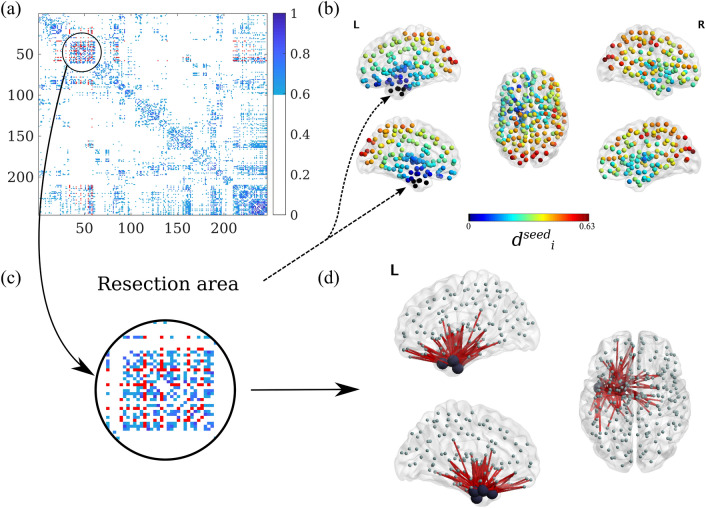
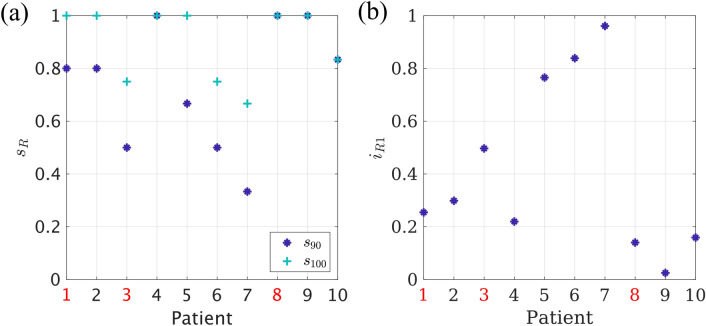
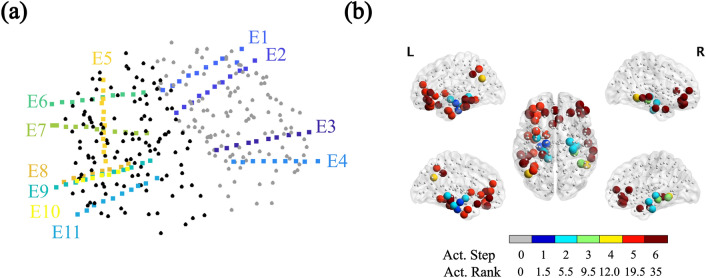
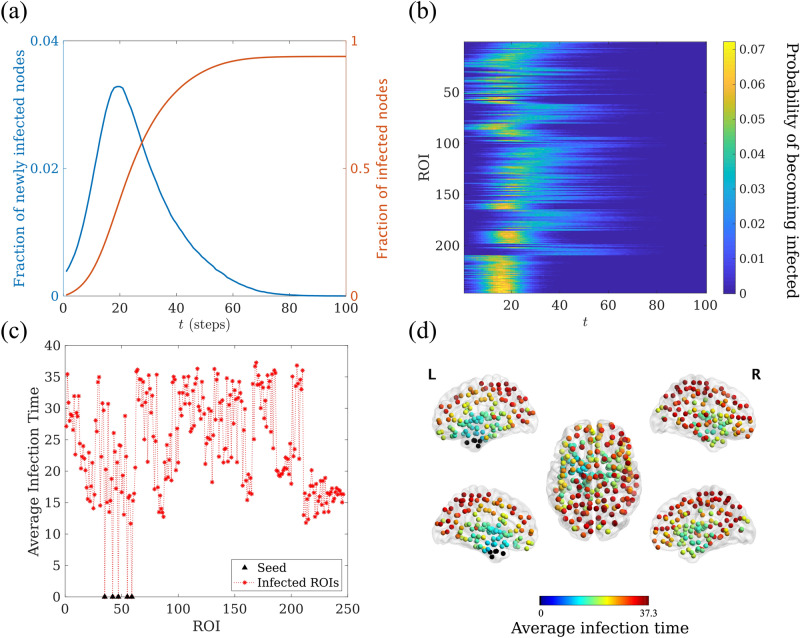
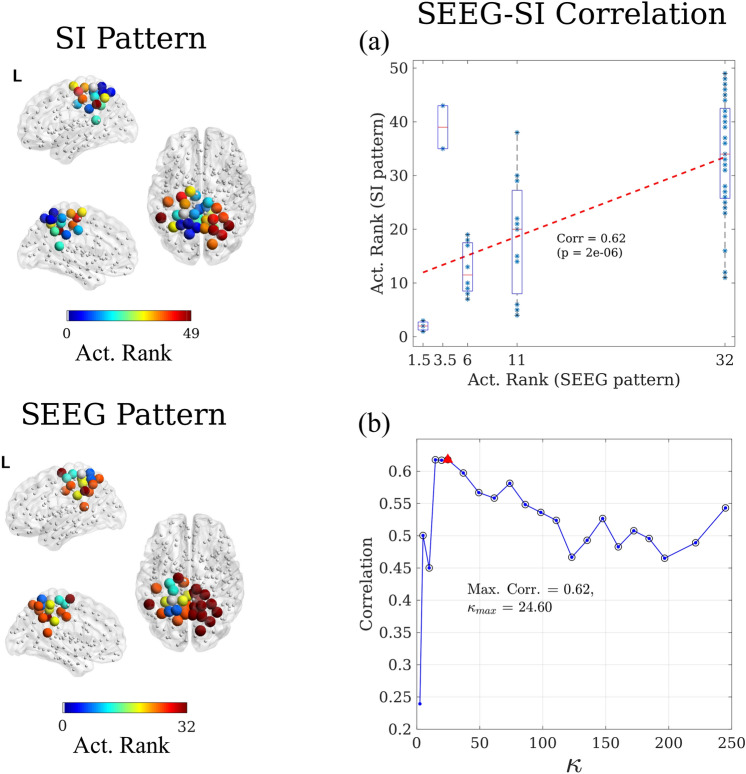
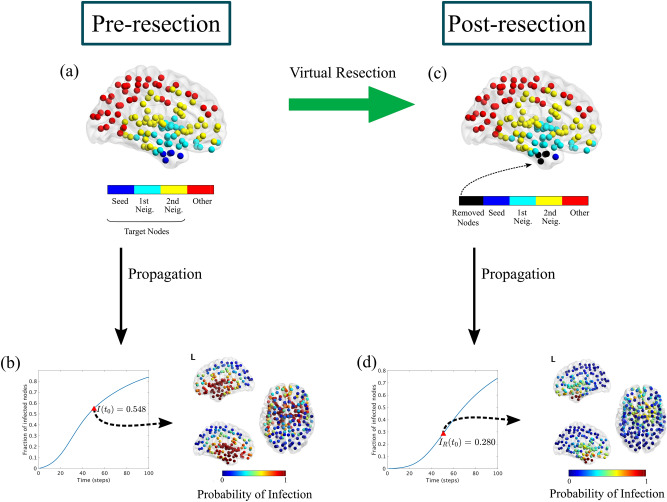
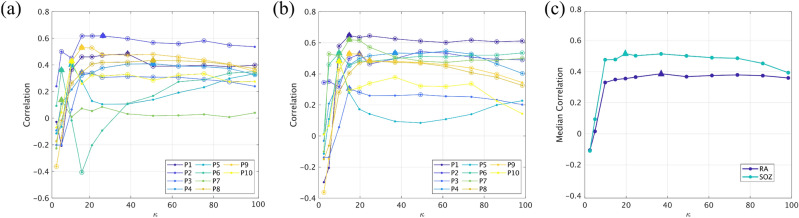
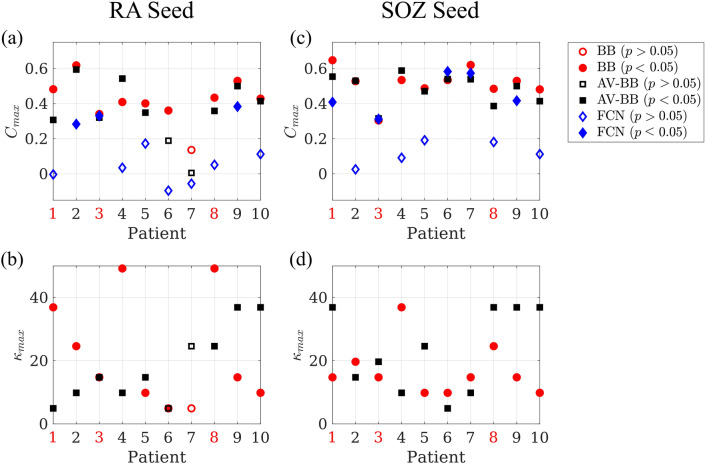
Epilepsy surgery is the treatment of choice for drug-resistant epilepsy patients. However, seizure-freedom is currently achieved in only 2/3 of the patients after surgery. In this study we have developed an individualized computational model based on MEG brain networks to explore seizure propagation and the efficacy of different virtual resections. Eventually, the goal is to obtain individualized models to optimize resection strategy and outcome. We have modelled seizure propagation as an epidemic process using the susceptible-infected (SI) model on individual brain networks derived from presurgical MEG. We included 10 patients who had received epilepsy surgery and for whom the surgery outcome at least one year after surgery was known. The model parameters were tuned in in order to reproduce the patient-specific seizure propagation patterns as recorded with invasive EEG. We defined a personalized search algorithm that combined structural and dynamical information to find resections that maximally decreased seizure propagation for a given resection size. The optimal resection for each patient was defined as the smallest resection leading to at least a 90% reduction in seizure propagation. The individualized model reproduced the basic aspects of seizure propagation for 9 out of 10 patients when using the resection area as the origin of epidemic spreading, and for 10 out of 10 patients with an alternative definition of the seed region. We found that, for 7 patients, the optimal resection was smaller than the resection area, and for 4 patients we also found that a resection smaller than the resection area could lead to a 100% decrease in propagation. Moreover, for two cases these alternative resections included nodes outside the resection area. Epidemic spreading models fitted with patient specific data can capture the fundamental aspects of clinically observed seizure propagation, and can be used to test virtual resections in silico. Combined with optimization algorithms, smaller or alternative resection strategies, that are individually targeted for each patient, can be determined with the ultimate goal to improve surgery outcome. MEG-based networks can provide a good approximation of structural connectivity for computational models of seizure propagation, and facilitate their clinical use.
癫痫手术是耐药性癫痫患者的首选治疗方法。然而,手术后只有 2/3 的患者达到无癫痫发作。在这项研究中,我们基于 MEG 脑网络开发了一种个体化的计算模型,以探索癫痫发作的传播和不同虚拟切除的效果。最终的目标是获得个体化的模型来优化切除策略和结果。我们将癫痫发作的传播建模为个体脑网络上的易感染-感染(SI)模型,这些脑网络来自术前 MEG。我们纳入了 10 名接受过癫痫手术且术后至少一年手术效果已知的患者。我们调整了模型参数,以重现具有侵袭性 EEG 记录的患者特定的癫痫发作传播模式。我们定义了一种个性化的搜索算法,该算法结合了结构和动力学信息,以找到在给定切除尺寸下最大程度减少癫痫发作传播的切除。对于每个患者,最佳切除定义为导致癫痫发作传播减少至少 90%的最小切除。当使用切除区域作为流行传播的起源时,个体化模型可以为 10 名患者中的 9 名重现 90%的癫痫发作传播的基本方面,对于 10 名患者中的 10 名使用替代种子区域定义。我们发现,对于 7 名患者,最佳切除小于切除区域,对于 4 名患者,我们还发现,切除小于切除区域可以导致传播完全减少。此外,对于两种情况,这些替代切除包括切除区域之外的节点。基于 MEG 的网络可以为癫痫发作传播的计算模型提供结构连接的良好近似,并且可以用于计算机上测试虚拟切除。结合优化算法,可以确定针对每个患者的个体化的更小或替代切除策略,最终目标是提高手术效果。