Department of Anesthesiology, Taipei Veterans General Hospital, Beitou Dist., Taipei, 11217, Taiwan.
School of Medicine, National Yang Ming Chiao Tung University, Hsinchu, 30010, Taiwan.
Sci Rep. 2022 Mar 8;12(1):4041. doi: 10.1038/s41598-022-08035-0.
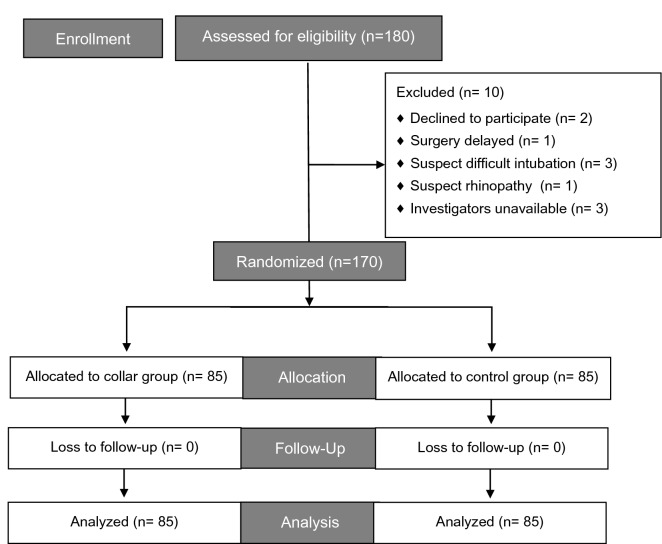
GlideScope-assisted nasotracheal intubation (NTI) has been proposed as an alternative to difficult orotracheal intubation for critical patients or those under cervical immobilization. We evaluated the difficulty of performing NTI using GlideScope under cervical orthosis. A total of 170 patients scheduled for elective cervical spinal surgery that required NTI were randomized to receive cervical immobilization using a cervical collar (collar group) or no cervical immobilization at all (control group) before anesthetic induction (group assignment at 1:1 ratio). All NTI during anesthetic induction were performed using the GlideScope. The primary outcome was time to intubation. The secondary outcomes were ease of intubation, including the necessity of auxiliary manipulations to assist intubation, and the nasotracheal intubation difficulty scale (nasoIDS). An exploratory analysis identified morphometric parameters as predictors of time to intubation, the necessity of auxiliary manipulations, and a nasoIDS score ≥ 4. For time to intubation, the mean difference (collar group-control) was - 4.19 s, with a 95% confidence interval (CI) of - 13.9 to 5.52 that lay within our defined equivalence margin of 16 s. Multivariate regressions precluded the association of cervical immobilization with a necessity for auxiliary manipulations (adjusted odds ratio [aOR] 0.53, 95% CI [0.26-1.09], P = 0.083) and a nasoIDS ≥ 4 (aOR 0.94 [0.84-1.05], P = 0.280). Among all morphometric parameters, the upper lip bite test class was predictive of a longer time to intubation (all analyses relative to class 1, 14 s longer for class 2, P = 0.032; 24 s longer for class 3, P = 0.070), increased necessity for auxiliary manipulation (aOR 2.29 [1.06-4.94], P = 0.036 for class 2; aOR 6.12 [1.04-39.94], P = 0.045 for class 3), and nasoIDS ≥ 4 (aOR 1.46 [1.14-1.89], P = 0.003 for class 3).The present study demonstrated that GlideScope achieved NTI in patients with or without cervical immobilization equivalently with respect to intubation time and ease.
GlideScope 辅助经鼻气管插管(NTI)已被提议作为困难或经口气管插管的替代方法,用于重症患者或颈椎固定患者。我们评估了颈椎固定下使用 GlideScope 进行 NTI 的难度。总共 170 名计划行颈椎手术且需要 NTI 的患者被随机分配在麻醉诱导前使用颈圈(颈圈组)或不使用颈圈(对照组)进行颈椎固定(1:1 比例分组)。所有麻醉诱导期间的 NTI 均使用 GlideScope 进行。主要结局是插管时间。次要结局是插管的难易程度,包括辅助插管操作的必要性,以及经鼻插管困难量表(nasoIDS)。探索性分析确定了形态计量学参数作为插管时间、辅助操作必要性和 nasoIDS 评分≥4 的预测因素。对于插管时间,颈圈组与对照组的平均差值为-4.19 秒,95%置信区间(CI)为-13.9 至 5.52,在我们定义的 16 秒等效边界内。多变量回归排除了颈椎固定与辅助操作必要性(调整优势比[aOR]0.53,95%CI[0.26-1.09],P=0.083)和 nasoIDS≥4(aOR 0.94 [0.84-1.05],P=0.280)之间的关联。在所有形态计量学参数中,上唇咬测试分级与插管时间延长相关(相对于分级 1,分级 2 长 14 秒,P=0.032;分级 3 长 24 秒,P=0.070),辅助操作的必要性增加(aOR 2.29 [1.06-4.94],P=0.036 分级 2;aOR 6.12 [1.04-39.94],P=0.045 分级 3),以及 nasoIDS≥4(aOR 1.46 [1.14-1.89],P=0.003 分级 3)。本研究表明,在插管时间和插管难易程度方面,GlideScope 在有或无颈椎固定的患者中实现 NTI 的效果相当。