Department of Cardiology, Sahlgrenska University Hospital, Gothenburg, 413 45, Sweden.
Institute of Medicine, University of Gothenburg, Gothenburg, Sweden.
ESC Heart Fail. 2022 Jun;9(3):1812-1822. doi: 10.1002/ehf2.13875. Epub 2022 Mar 8.
Ischaemic coronary artery disease (CAD) remains the leading cause of mortality globally due to sudden death and heart failure (HF). Invasive coronary angiography (CAG) is the gold standard for evaluating the presence and severity of CAD. Our objective was to assess temporal trends in CAG utilization, patient characteristics, and prognosis in HF patients undergoing CAG at a national level.
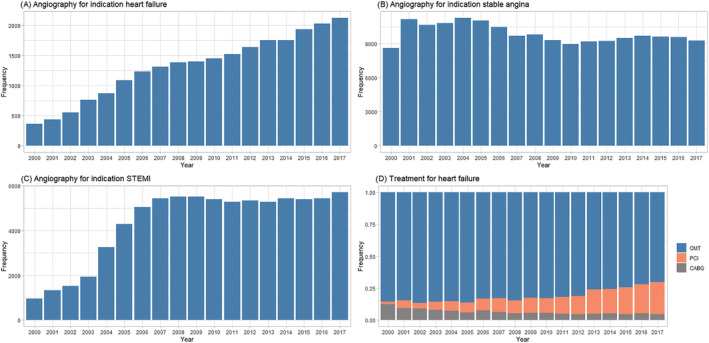
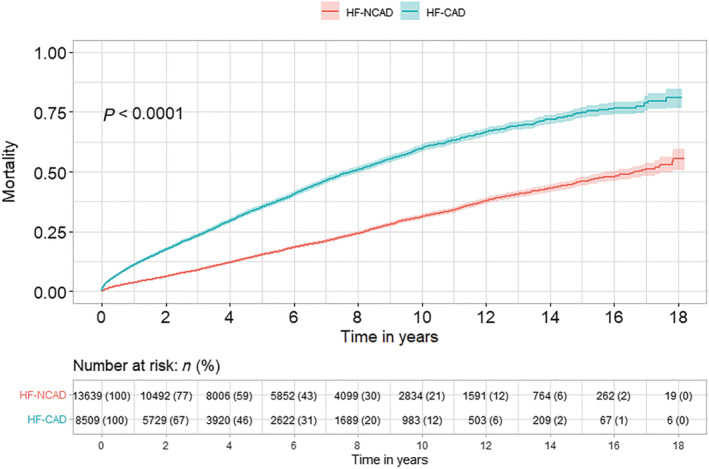
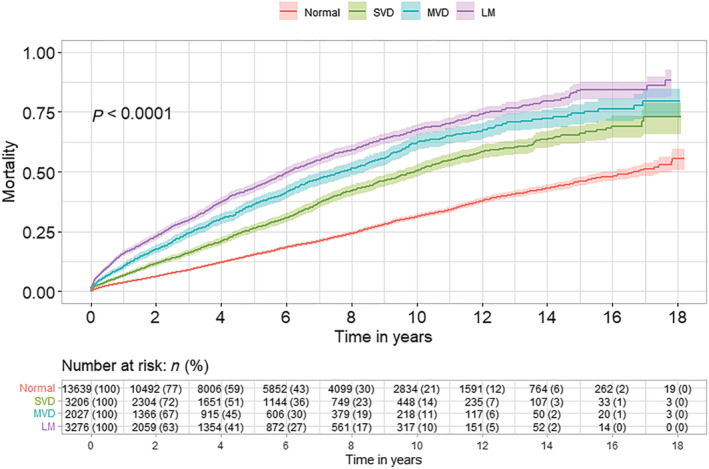
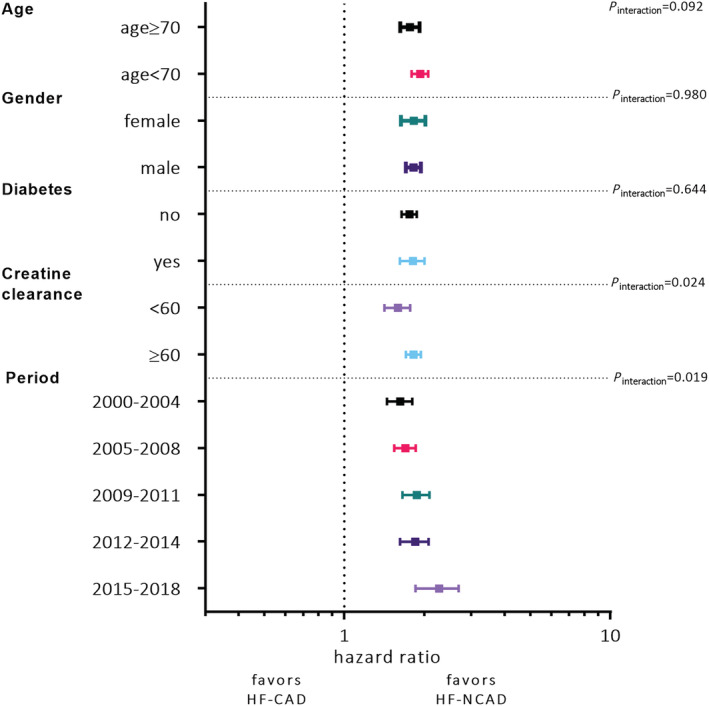
We used data from the Swedish Coronary Angiography and Angioplasty Registry. Data on all patients undergoing CAG for HF indication in Sweden between 2000 and 2018 were collected and analysed. Long-term survival was estimated with multivariable Cox proportional hazards regression adjusted for differences in patient characteristics. In total, 22 457 patients (73% men) with mean age 64.2 ± 11.3 years were included in the study. The patients were increasingly older with more comorbidities over time. The number of CAG specifically for HF indication increased by 5.5% per calendar year (P < 0.001). No such increase was seen for indications angina pectoris and ST-elevation myocardial infarction. A normal CAG or non-obstructive CAD was reported in 63.2% (HF-NCAD), and 36.8% had >50% diameter stenosis in one or more coronary arteries (HF-CAD). The median follow-up time was 3.6 years in HF-CAD and 5 years in HF-NCAD. Age and sex-adjusted survival improved linearly by 1.3% per calendar year in all patients. Compared with HF-NCAD, long-term mortality was higher in HF-CAD patients. The risk of death increased with the increasing severity of CAD. Compared with HF-NCAD, the risk estimate in patients with a single-vessel disease was higher [hazard ratio (HR) 1.3; 95% confidence interval (CI) 1.20-1.41; P < 0.001], a multivessel disease without the involvement of left main coronary artery (HR 1.72; 95% CI 1.58-1.88; P < 0.001), and with left main disease (HR 2.02; 95% CI 1.88-2.18; P < 0.001). The number of HF patients undergoing revascularization with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) increased by 7.5% (P < 0.001) per calendar year. The majority (53.4%) of HF-CAD patients were treated medically, while a minority (46.6%) were referred for revascularization with PCI or CABG. Compared with patients treated with PCI, the proportion of patients treated medically or with CABG decreased substantially (P < 0.001).
Over 18 years, the number of patients with HF undergoing CAG has increased substantially. Expanded utilization of CAG increased the number of HF patients treated with percutaneous coronary intervention and coronary artery bypass surgery. Long-term survival improved in all HF patients despite a steady increase of elderly patients with comorbidities.
由于突发性死亡和心力衰竭(HF),缺血性冠状动脉疾病(CAD)仍然是全球主要的死亡原因。有创冠状动脉造影(CAG)是评估 CAD 存在和严重程度的金标准。我们的目的是评估全国范围内因 HF 而行 CAG 的患者的 CAG 利用情况、患者特征和预后的时间趋势。
我们使用了瑞典冠状动脉血管造影和血管成形术登记处的数据。收集并分析了 2000 年至 2018 年间瑞典所有因 HF 指征而行 CAG 的患者的数据。采用多变量 Cox 比例风险回归分析,根据患者特征的差异调整长期生存率。共有 22457 名(73%为男性)平均年龄 64.2±11.3 岁的患者纳入研究。随着时间的推移,患者年龄越来越大,合并症也越来越多。专门用于 HF 指征的 CAG 数量每年增加 5.5%(P<0.001)。心绞痛和 ST 段抬高型心肌梗死的指征并没有出现这种增加。63.2%(HF-NCAD)报告了正常 CAG 或非阻塞性 CAD,36.8%的患者在一条或多条冠状动脉中存在>50%的直径狭窄(HF-CAD)。HF-CAD 的中位随访时间为 3.6 年,HF-NCAD 为 5 年。所有患者的年龄和性别调整后的生存率每年线性提高 1.3%。与 HF-NCAD 相比,HF-CAD 患者的长期死亡率更高。随着 CAD 严重程度的增加,死亡风险也会增加。与 HF-NCAD 相比,单支血管疾病患者的风险估计值更高(HR 1.3;95%CI 1.20-1.41;P<0.001),无左主干冠状动脉受累的多支血管疾病(HR 1.72;95%CI 1.58-1.88;P<0.001)和左主干疾病(HR 2.02;95%CI 1.88-2.18;P<0.001)。每年接受经皮冠状动脉介入治疗(PCI)或冠状动脉旁路移植术(CABG)的 HF 患者数量增加了 7.5%(P<0.001)。大多数(53.4%)HF-CAD 患者接受药物治疗,而少数(46.6%)患者接受 PCI 或 CABG 血运重建治疗。与接受 PCI 治疗的患者相比,接受药物治疗或 CABG 治疗的患者比例大幅下降(P<0.001)。
在 18 年多的时间里,因 HF 而行 CAG 的患者数量大幅增加。有创冠状动脉造影的广泛应用增加了接受经皮冠状动脉介入治疗和冠状动脉旁路移植术治疗的 HF 患者数量。尽管老年合并症患者数量不断增加,但所有 HF 患者的长期生存率都有所提高。