Takahashi Akira, Miyauchi Takamasa, Tatsumoto Narihito, Lin Mercury Y, Hou Jean, Doi Toshiki, Masaki Takao, Yamashita Michifumi
Department of Pathology and Laboratory Medicine, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
Department of Nephrology, Hiroshima University Hospital, Hiroshima, Japan.
Clin Kidney J. 2021 Jan 11;14(9):2090-2100. doi: 10.1093/ckj/sfaa276. eCollection 2021 Sep.
Nephropathy in patients with thymic diseases such as thymoma and myasthenia gravis (MG) is rare and has been described mostly as isolated case reports. Here we evaluate a series of kidney biopsies from patients with thymoma and/or MG from a single institution in order to better define the spectrum and relative frequencies of thymic disease-associated nephropathies.
We conducted a retrospective case series study of 32 462 native kidney biopsies from January 2005 through December 2019 at Cedars-Sinai Medical Center, Los Angeles, CA, USA.
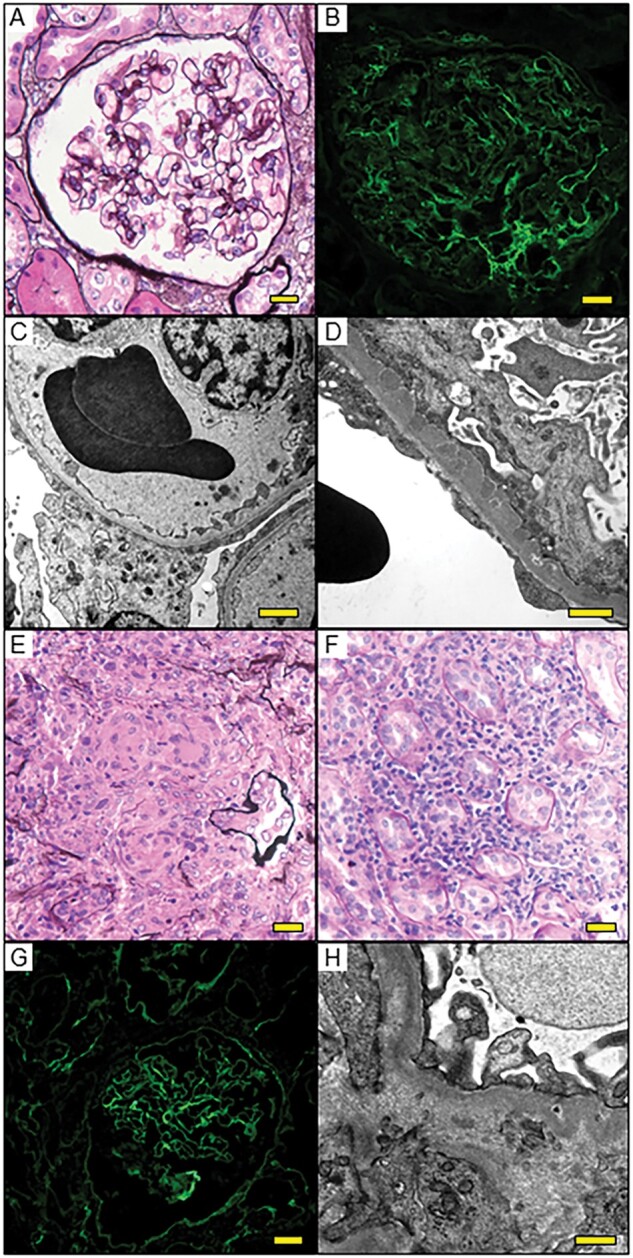
Twenty-four biopsy specimens (0.07%) from patients with a history of thymoma and/or MG were identified. Two patients had repeat biopsies. The most common pathologic diagnosis that could be immunologically attributed to thymic disease was minimal change disease (MCD; 45%), followed by tubulointerstitial nephritis (TIN; 14%), immune complex (IC)-mediated glomerulonephritis (9%), membranous nephropathy (5%) and immunoglobulin A (IgA) nephropathy (5%). Interestingly, 50% of the MCD and 67% of TIN cases concomitantly showed mild IgG-dominant IC deposition in mesangial areas and/or in tubular basement membranes. In the two patients with repeat biopsies, mild mesangial IC deposition developed in the MCD patient but disappeared in the TIN patient with the second biopsy. Pathologic diagnoses unlikely related to the underlying thymic disease were diabetic glomerulosclerosis (9%), acute tubular necrosis (9%) and monoclonal Ig deposition disease (5%).
Thymic disease is associated with a wide spectrum of kidney diseases affecting the glomerular and tubulointerstitial compartments, often with low-grade IC deposition. These findings suggest a role of immunologic dysregulation in the pathogenesis of thymic disease-associated nephropathy.
胸腺疾病(如胸腺瘤和重症肌无力)患者的肾病较为罕见,大多以个案报道形式呈现。在此,我们评估了来自同一机构的一系列胸腺瘤和/或重症肌无力患者的肾脏活检样本,以更好地明确胸腺疾病相关肾病的范围和相对频率。
我们对2005年1月至2019年12月在美国加利福尼亚州洛杉矶雪松西奈医疗中心进行的32462例自体肾脏活检进行了回顾性病例系列研究。
共识别出24例有胸腺瘤和/或重症肌无力病史患者的活检样本(0.07%)。两名患者进行了重复活检。在免疫方面可归因于胸腺疾病的最常见病理诊断是微小病变性肾病(MCD;45%),其次是肾小管间质性肾炎(TIN;14%)、免疫复合物(IC)介导的肾小球肾炎(9%)、膜性肾病(5%)和免疫球蛋白A(IgA)肾病(5%)。有趣的是,50%的MCD病例和67%的TIN病例在系膜区和/或肾小管基底膜同时出现轻度IgG为主的IC沉积。在两名进行重复活检的患者中,MCD患者出现了轻度系膜IC沉积,但在第二次活检时TIN患者的沉积消失。与潜在胸腺疾病不太可能相关的病理诊断为糖尿病肾小球硬化(9%)、急性肾小管坏死(9%)和单克隆Ig沉积病(5%)。
胸腺疾病与多种影响肾小球和肾小管间质的肾脏疾病相关,常伴有低度IC沉积。这些发现提示免疫失调在胸腺疾病相关肾病发病机制中起作用。