Stephens Robert J, Evans Erin M, Pajor Michael J, Pappal Ryan D, Egan Haley M, Wei Max, Hayes Hunter, Morris Jason A, Becker Nicholas, Roberts Brian W, Kollef Marin H, Mohr Nicholas M, Fuller Brian M
Barnes-Jewish Hospital.
University of Iowa.
Res Sq. 2022 Mar 1:rs.3.rs-1389892. doi: 10.21203/rs.3.rs-1389892/v1.
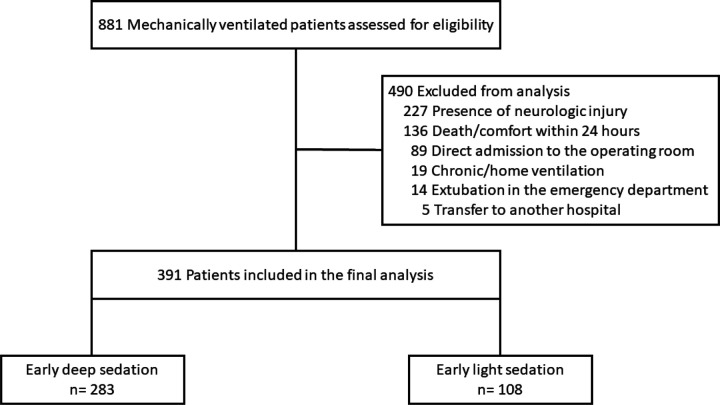
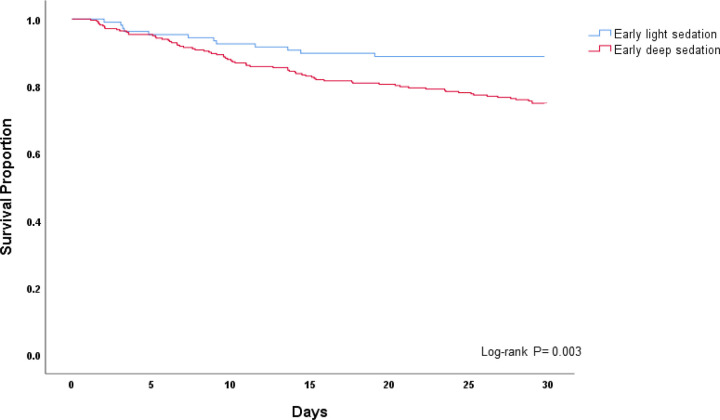
: Mechanically ventilated patients have experienced greater periods of prolonged deep sedation during the coronavirus disease (COVID-19) pandemic. Multiple studies from the pre-COVID era demonstrate that early deep sedation is associated with worse outcome. Despite this, there is a lack of data on sedation depth and its impact on outcome for mechanically ventilated patients during the COVID-19 pandemic. We sought to characterize the emergency department (ED) and intensive care unit (ICU) sedation practices during the COVID-19 pandemic, and to determine if early deep sedation was associated with worse clinical outcomes. : Dual-center, retrospective cohort study conducted over six months (March - August, 2020), involving consecutive, mechanically ventilated adults. All sedation-related data during the first 48 hours were collected. Deep sedation was defined as Richmond Agitation-Sedation Scale of -3 to -5 or Riker Sedation-Agitation Scale of 1 - 3. To examine impact of early sedation depth on hospital mortality (primary outcome) we used a multivariable logistic regression model. Secondary outcomes included ventilator-, ICU-, and hospital-free days. : 391 patients were studied, and 283 (72.4%) experienced early deep sedation. Deeply sedated patients received higher cumulative doses of fentanyl, propofol, midazolam, and ketamine when compared to light sedation. Deep sedation patients experienced fewer ventilator-, ICU-, and hospital-free days, and greater mortality (30.4% versus 11.1%) when compared to light sedation ( < 0.01 for all). After adjusting for confounders, early deep sedation remained significantly associated with higher mortality (adjusted OR 3.44; 95% CI 1.65 - 7.17; p <0.01). These results were stable in the subgroup of patients with COVID-19. : The management of sedation for mechanically ventilated patients in the ICU has changed during the COVID pandemic. Early deep sedation is common and independently associated with worse clinical outcomes. A protocol-driven approach to sedation, targeting light sedation as early as possible, should continue to remain the default approach. : Not applicable.
在冠状病毒病(COVID-19)大流行期间,接受机械通气的患者经历深度镇静的时间更长。COVID-19大流行之前的多项研究表明,早期深度镇静与更差的预后相关。尽管如此,关于COVID-19大流行期间机械通气患者的镇静深度及其对预后的影响,仍缺乏数据。我们试图描述COVID-19大流行期间急诊科(ED)和重症监护病房(ICU)的镇静实践,并确定早期深度镇静是否与更差的临床结局相关。:进行了为期六个月(2020年3月至8月)的双中心回顾性队列研究,纳入连续的接受机械通气的成年人。收集了前48小时内所有与镇静相关的数据。深度镇静定义为里士满躁动镇静量表评分为-3至-5或里克镇静躁动量表评分为1至3。为了研究早期镇静深度对医院死亡率(主要结局)的影响,我们使用了多变量逻辑回归模型。次要结局包括无呼吸机天数、无ICU天数和无住院天数。:共研究了391例患者,其中283例(72.4%)经历了早期深度镇静。与轻度镇静患者相比,深度镇静患者接受的芬太尼、丙泊酚、咪达唑仑和氯胺酮的累积剂量更高。与轻度镇静患者相比,深度镇静患者的无呼吸机天数、无ICU天数和无住院天数更少,死亡率更高(30.4%对11.1%)(所有p均<0.01)。在对混杂因素进行调整后,早期深度镇静仍与较高的死亡率显著相关(调整后的比值比为3.44;95%置信区间为1.65 - 7.17;p<0.01)。这些结果在COVID-19患者亚组中是稳定的。:在COVID大流行期间,ICU中机械通气患者的镇静管理发生了变化。早期深度镇静很常见,且与更差的临床结局独立相关。以尽可能早地实现轻度镇静为目标的基于方案的镇静方法,应继续作为默认方法。:不适用。