Department of Cardiovascular Medicine, Mayo Clinic, Rochester, Minnesota, United States of America.
Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, Minnesota, United States of America.
PLoS One. 2022 Mar 9;17(3):e0262053. doi: 10.1371/journal.pone.0262053. eCollection 2022.
Echocardiographic findings vary with shock severity, as defined by the Society for Cardiovascular Angiography and Intervention (SCAI) shock stage. Left ventricular stroke work index (LVSWI) measured by transthoracic echocardiography (TTE) can predict mortality in the cardiac intensive care unit (CICU). We sought to determine whether LVSWI could refine mortality risk stratification by the SCAI shock classification in the CICU.
We included consecutive CICU patients from 2007 to 2015 with TTE data available to calculate the LVSWI, specifically the mean arterial pressure, stroke volume index and medial mitral E/e' ratio. In-hospital mortality as a function of LVSWI was evaluated across the SCAI shock stages using logistic regression, before and after multivariable adjustment.
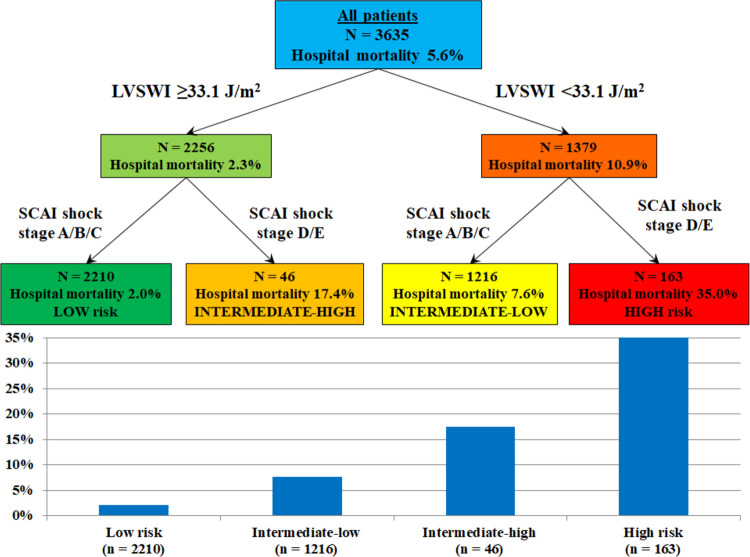
We included 3635 unique CICU patients, with a mean age of 68.1 ± 14.5 years (36.5% females); 61.1% of patients had an acute coronary syndrome. The LVSWI progressively decreased with increasing shock severity, as defined by increasing SCAI shock stage. A total of 203 (5.6%) patients died during hospitalization, with higher in-hospital mortality among patients with lower LVSWI (adjusted OR 0.66 per 10 J/m2 higher) or higher SCAI shock stage (adjusted OR 1.24 per each higher stage). A LVSWI <33 J/m2 was associated with higher adjusted in-hospital mortality, particularly among patients with shock (SCAI stages C, D and E).
The LVSWI by TTE noninvasively characterizes the severity of shock, including both systolic and diastolic parameters, and can identify low-risk and high-risk patients at each level of clinical shock severity.
超声心动图检查结果因心血管造影和介入学会(SCAI)休克分期定义的休克严重程度而异。经胸超声心动图(TTE)测量的左心室每搏功指数(LVSWI)可预测心脏重症监护病房(CICU)的死亡率。我们试图确定 LVSWI 是否可以通过 CICU 中的 SCAI 休克分类来细化死亡率风险分层。
我们纳入了 2007 年至 2015 年期间连续的 CICU 患者,这些患者均有 TTE 数据可用于计算 LVSWI,具体为平均动脉压、每搏量指数和中隔二尖瓣 E/e' 比值。使用逻辑回归评估 LVSWI 与 SCAI 休克分期的关系,分别在多变量调整前后进行评估。
我们纳入了 3635 例独特的 CICU 患者,平均年龄为 68.1 ± 14.5 岁(36.5%为女性);61.1%的患者患有急性冠脉综合征。随着 SCAI 休克分期的增加,定义的休克严重程度逐渐增加,LVSWI 逐渐降低。共有 203(5.6%)名患者在住院期间死亡,LVSWI 越低(调整后的比值比每增加 10 J/m2 为 0.66)或 SCAI 休克分期越高(调整后的比值比每增加一个阶段为 1.24),住院死亡率越高。LVSWI <33 J/m2 与较高的调整后住院死亡率相关,特别是在休克患者中(SCAI 分期 C、D 和 E)。
TTE 测量的 LVSWI 无创性地描述了休克的严重程度,包括收缩和舒张参数,并可在每个临床休克严重程度水平识别低风险和高风险患者。