Li Chenghui, Bhatti Sajjad A, Ying Jun
Division of Pharmaceutical Evaluation and Policy, Department of Pharmacy Practice, College of Pharmacy, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA.
Internal Medicine Hematology-Oncology, College of Medicine, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA.
Cancers (Basel). 2022 Feb 23;14(5):1145. doi: 10.3390/cancers14051145.
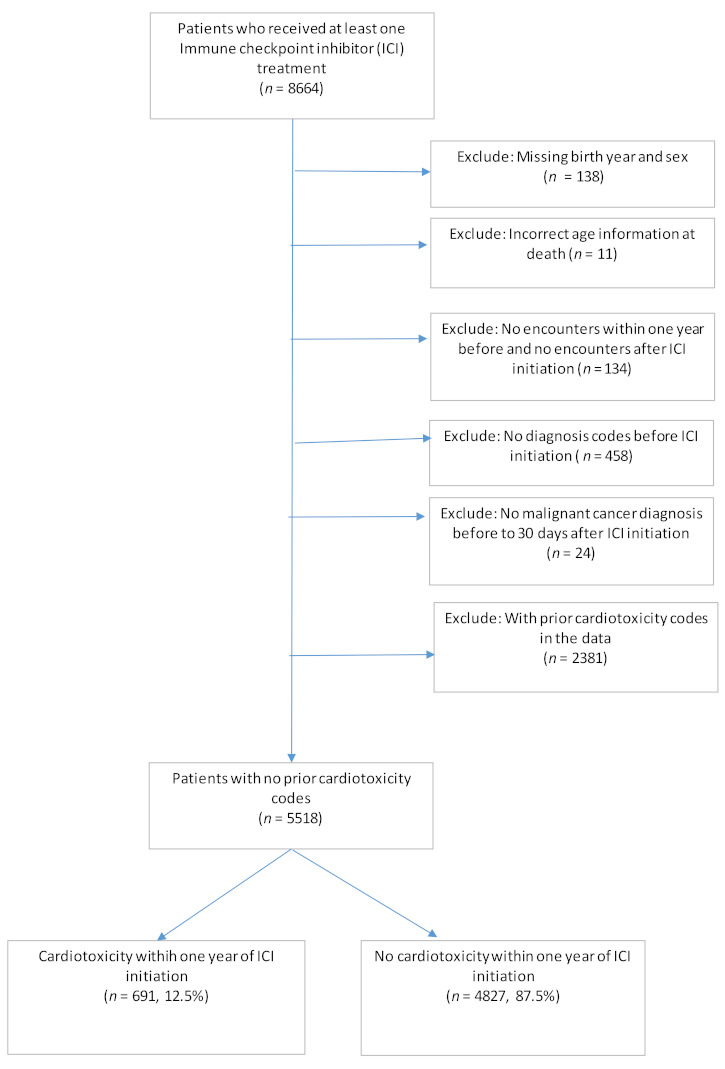
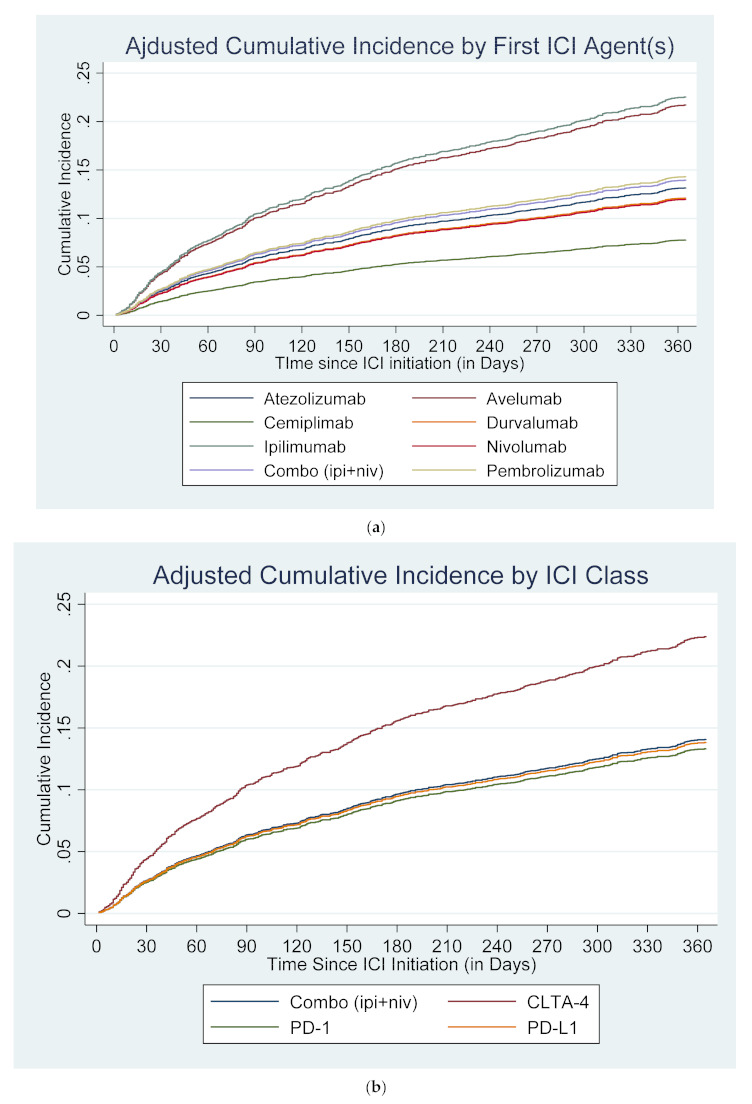
Large population-based studies examining differences in ICI-associated cardiotoxicity across cancer types and agents are limited. Data of 5518 cancer patients who received at least one cycle of ICIs were extracted from a large network of health care organizations. ICI treatment groups were classified by the first ICI agent(s) (ipilimumab, nivolumab, pembrolizumab, cemiplimab, avelumab, atezolizumab, or durvalumab) or its class (PD-1 inhibitors, PD-L1 inhibitors, CTLA4-inhibitors, or their combination (ipilimumab + nivolumab)). Time to first cardiac adverse event (CAE) (arrhythmia, acute myocardial infarction, myocarditis, cardiomyopathy, or pericarditis) developed within one year after ICI initiation was analyzed using a competing-risks regression model adjusting for ICI treatment groups, patient demographic and clinical characteristics, and cancer sites. By month 12, 12.5% developed cardiotoxicity. The most common cardiotoxicity was arrhythmia (9.3%) and 2.1% developed myocarditis. After adjusting for patient characteristics and cancer sites, patients who initiated on monotherapy with ipilimumab (adjusted Hazard Ratio (aHR): 2.00; 95% CI: 1.49−2.70; p < 0.001) or pembrolizumab (aHR: 1.21; 95% CI: 1.01−1.46; p = 0.040) had a higher risk of developing CAEs within one year compared to nivolumab monotherapy. Ipilimumab and pembrolizumab use may increase the risk of cardiotoxicity compared to other agents. Avelumab also estimated a highly elevated risk (aHR: 1.92; 95% CI: 0.85−4.34; p = 0.117) compared to nivolumab and other PD-L1 agents, although the estimate did not reach statistical significance, warranting future studies.
基于大规模人群的研究,考察不同癌症类型和药物之间ICI相关心脏毒性的差异,此类研究较为有限。从一个大型医疗保健组织网络中提取了5518名接受至少一个周期ICI治疗的癌症患者的数据。ICI治疗组根据首个ICI药物(伊匹木单抗、纳武单抗、帕博利珠单抗、西米普利单抗、阿维鲁单抗、阿替利珠单抗或度伐利尤单抗)或其类别(PD-1抑制剂、PD-L1抑制剂、CTLA4抑制剂或其组合(伊匹木单抗+纳武单抗))进行分类。使用竞争风险回归模型分析首次心脏不良事件(CAE)(心律失常、急性心肌梗死、心肌炎、心肌病或心包炎)在ICI开始后一年内发生的时间,并对ICI治疗组、患者人口统计学和临床特征以及癌症部位进行了调整。到第12个月时,12.5%的患者出现了心脏毒性。最常见的心脏毒性是心律失常(9.3%),2.1%的患者出现了心肌炎。在对患者特征和癌症部位进行调整后,与纳武单抗单药治疗相比,开始使用伊匹木单抗单药治疗的患者(调整后风险比(aHR):2.00;95%置信区间:1.49−2.70;p<0.001)或帕博利珠单抗单药治疗的患者(aHR:1.21;95%置信区间:1.01−1.46;p = 0.040)在一年内发生CAE的风险更高。与其他药物相比,使用伊匹木单抗和帕博利珠单抗可能会增加心脏毒性的风险。与纳武单抗和其他PD-L1药物相比,阿维鲁单抗估计风险也显著升高(aHR:1.92;95%置信区间:0.85−4.34;p = 0.117),尽管该估计未达到统计学意义,仍需进一步研究。