Tomaniak Mariusz, Neleman Tara, Ziedses des Plantes Anniek, Masdjedi Kaneshka, van Zandvoort Laurens J C, Kochman Janusz, den Dekker Wijnand K, Wilschut Jeroen M, Diletti Roberto, Kardys Isabella, Zijlstra Felix, Van Mieghem Nicolas M, Daemen Joost
Department of Cardiology, Erasmus University Medical Center, ThoraxCenter, 3000 CA Rotterdam, The Netherlands.
First Department of Cardiology, Medical University of Warsaw, 02-091 Warsaw, Poland.
J Clin Med. 2022 Mar 3;11(5):1397. doi: 10.3390/jcm11051397.
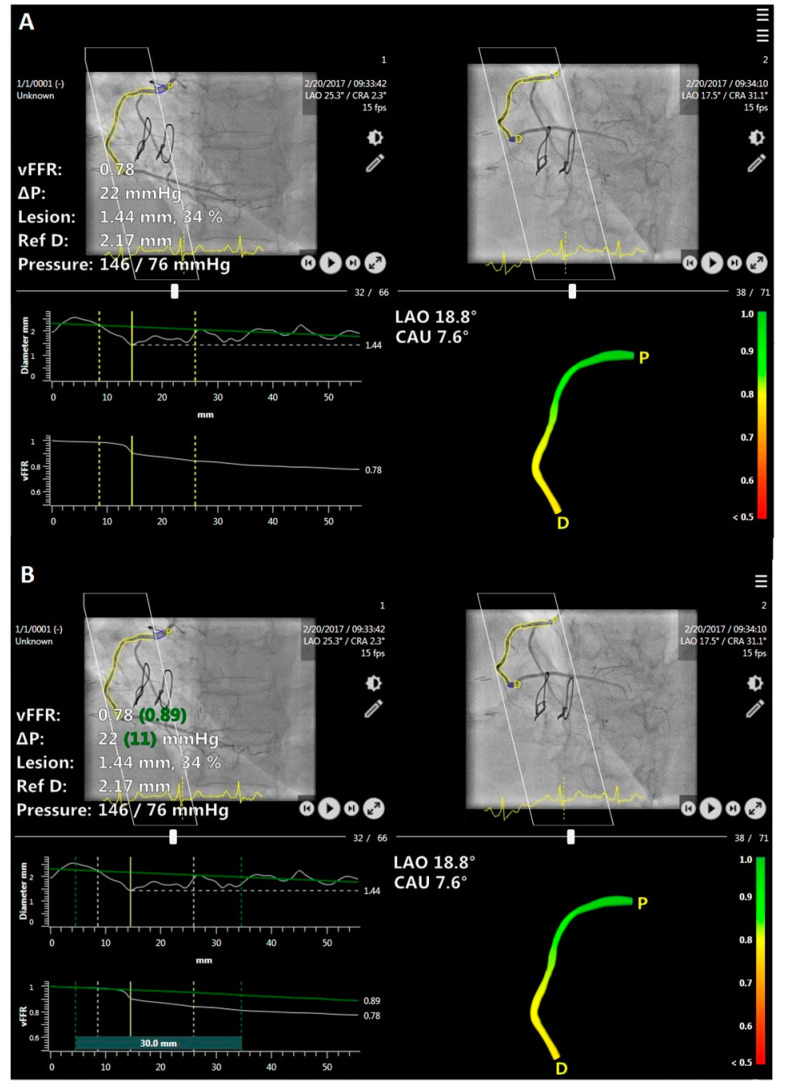
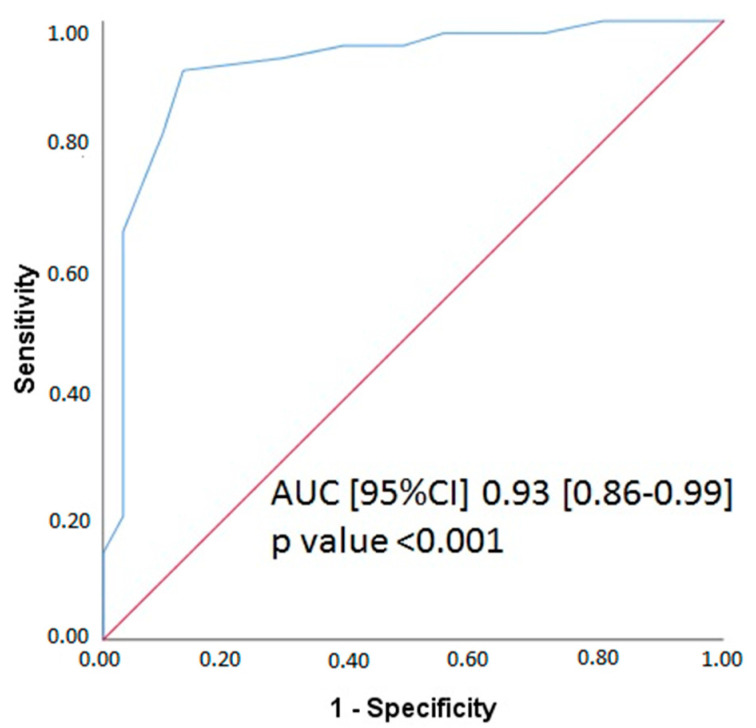
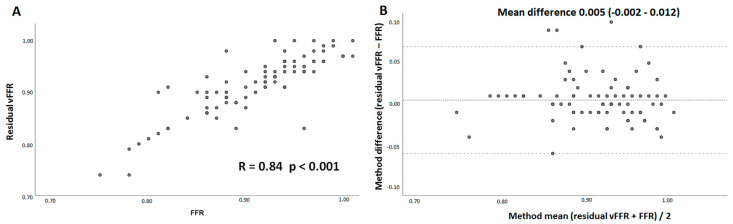
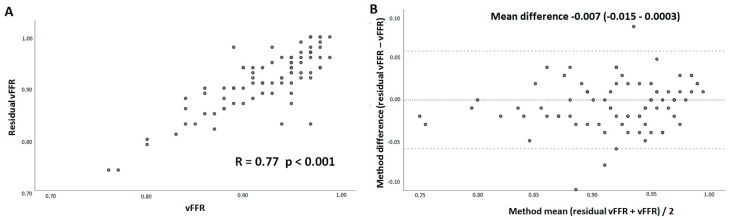
3D coronary angiography-based vessel fractional flow reserve (vFFR) proved to be an accurate diagnostic alternative to invasively measured pressure wire based fractional flow reserve (FFR). The ability to compute post-PCI vFFR using pre-PCI vFFR virtual stent analysis is unknown. We aimed to assess the feasibility and diagnostic accuracy of pre-PCI vFFR virtual stenting analysis (residual vFFR) with post-PCI FFR as a reference. This is an observational, single-center retrospective cohort study including consecutive patients from the FFR-SEARCH registry. We blindly calculated residual vFFR from pre-PCI angiograms and compared them to invasive pressure-wire based post-PCI FFR. Inclusion criteria involved presentation with either stable or unstable angina or non-ST elevation myocardial infarction (NSTEMI), ≥1 significant stenosis in one of the epicardial coronary arteries (percentage diameter stenosis of >70% by QCA or hemodynamically relevant stenosis with FFR ≤0.80) and pre procedural angiograms eligible for vFFR analysis. Exclusion criteria comprised patients with ST elevation myocardial infarction (STEMI), coronary bypass grafts, cardiogenic shock or severe hemodynamic instability. Eighty-one pre-PCI residual vFFR measurements were compared to post-PCI FFR and post-PCI vFFR measurements. Mean residual vFFR was 0.91 ± 0.06, mean post-PCI FFR 0.91 ± 0.06 and mean post-PCI vFFR was 0.92 ± 0.05. Residual vFFR showed a high linear correlation (r = 0.84) and good agreement (mean difference (95% confidence interval): 0.005 (−0.002−0.012)) with post-PCI FFR, as well as with post-PCI-vFFR (r = 0.77, mean difference −0.007 (−0.015−0.0003)). Residual vFFR showed good accuracy in the identification of lesions with post-PCI FFR < 0.90 (sensitivity 94%, specificity 71%, area under the curve (AUC) 0.93 (95% CI: 0.86−0.99), p < 0.001). Virtual stenting using vFFR provided an accurate estimation of post-PCI FFR and post-PCI vFFR. Further studies are needed to prospectively validate a vFFR-guided PCI strategy.
基于三维冠状动脉造影的血管血流储备分数(vFFR)被证明是一种准确的诊断方法,可替代基于有创压力导丝测量的血流储备分数(FFR)。利用PCI术前vFFR虚拟支架分析来计算PCI术后vFFR的能力尚不清楚。我们旨在评估以PCI术后FFR为参考的PCI术前vFFR虚拟支架分析(残余vFFR)的可行性和诊断准确性。这是一项观察性、单中心回顾性队列研究,纳入了FFR-SEARCH注册研究中的连续患者。我们从PCI术前血管造影中盲目计算残余vFFR,并将其与基于有创压力导丝的PCI术后FFR进行比较。纳入标准包括表现为稳定型或不稳定型心绞痛或非ST段抬高型心肌梗死(NSTEMI)、一支心外膜冠状动脉中存在≥1处严重狭窄(定量冠状动脉造影显示直径狭窄百分比>70%或FFR≤0.80的血流动力学相关狭窄)以及符合vFFR分析条件的术前血管造影。排除标准包括ST段抬高型心肌梗死(STEMI)患者、冠状动脉旁路移植术患者、心源性休克或严重血流动力学不稳定患者。将81例PCI术前残余vFFR测量值与PCI术后FFR及PCI术后vFFR测量值进行比较。平均残余vFFR为0.91±0.06,平均PCI术后FFR为0.91±0.06,平均PCI术后vFFR为0.92±0.05。残余vFFR与PCI术后FFR以及PCI术后vFFR均显示出高度线性相关性(r = 0.84)和良好的一致性(平均差异(95%置信区间):0.005(-0.002-0.012)),与PCI术后vFFR的相关性为r = 0.77,平均差异为-0.007(-0.015-0.0003)。残余vFFR在识别PCI术后FFR<0.90的病变方面显示出良好的准确性(敏感性94%,特异性71%,曲线下面积(AUC)0.93(95%CI:0.86-0.99),p<0.001)。使用vFFR进行虚拟支架置入可准确估计PCI术后FFR和PCI术后vFFR。需要进一步的研究来前瞻性验证vFFR指导的PCI策略。