Department of Cardiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Zhejiang, China.
Department of Cardiology, Barts Heart Centre, Barts Health NHS Trust, London, UK.
Int J Cardiovasc Imaging. 2021 May;37(5):1491-1501. doi: 10.1007/s10554-020-02133-8. Epub 2021 Jan 16.
Angiography derived FFR reveals good performance in assessing intermediate coronary stenosis. However, its performance under contemporary low X-ray frame and pulse rate settings is unknown. We aim to validate the feasibility and performance of quantitative flow ratio (QFR) and vessel fractional flow reserve (vFFR) under such angiograms.
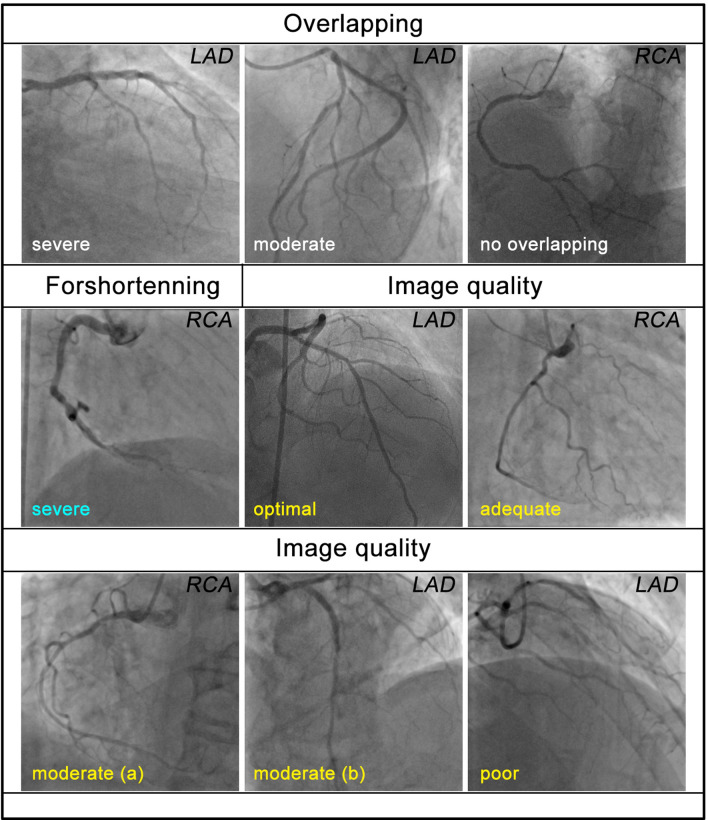
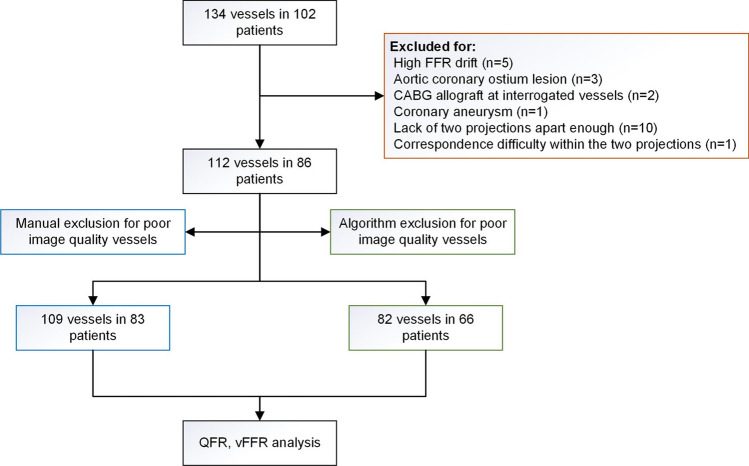
This was an observational, retrospective, single center cohort study. 134 vessels in 102 patients, with angiograms acquired under 7.5fps and 7pps mode, were enrolled. QFR (fQFR and cQFR) and vFFR were validated with FFR as the gold standard. A conventional manual and a newly developed algorithmic exclusion method (M and A group) were both evaluated for identification of poor-quality angiograms.
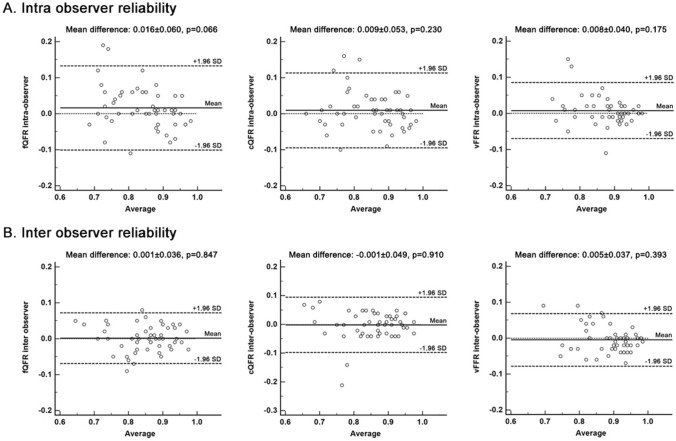
Good agreement between QFR/vFFR and FFR were observed in both M and A group, except for vFFR in the M group. The correlation coefficients between fQFR/cQFR/vFFR and FFR were 0.6242, 0.5888, 0.4089 in the M group, with r significantly lower than r (p = 0.0303), and 0.7055, 0.6793, 0.5664 in the A group, respectively. AUCs of detecting lesions with FFR ≤ 0.80 were 0.852 (95% CI 0.722-0.913), 0.858 (95% CI 0.778-0.917), 0.682 (95% CI 0.586-0.768), for fQFR/cQFR/vFFR in the M group, while vFFR performed poorer than fQFR (p = 0.0063) and cQFR (p = 0.0054). AUCs were 0.898 (95% CI 0.811-0.945), 0.892 (95% CI 0.803-0.949), 0.843 (95% CI 0.746-0.914) for fQFR/cQFR/vFFR in the A group. AUC was significantly higher in the A group than that in the M group (p = 0.0399).
QFR/vFFR assessment is feasible under 7.5fps and 7pps angiography, where cQFR showed no advantage compared to fQFR. Our newly developed algorithmic exclusion method could be a better method of selecting angiograms with adequate quality for angiography derived FFR assessment.
血管造影衍生的 FFR 在心外膜狭窄的评估中表现良好。然而,在当代低 X 射线帧率和脉冲率设置下,其性能尚不清楚。我们旨在验证定量血流比(QFR)和血管分数血流储备(vFFR)在这种血管造影下的可行性和性能。
这是一项观察性、回顾性、单中心队列研究。纳入了 102 例患者的 134 支血管,这些血管的血管造影是在 7.5fps 和 7pps 模式下采集的。使用 FFR 作为金标准对 QFR(fQFR 和 cQFR)和 vFFR 进行验证。评估了一种传统的手动和新开发的算法排除方法(M 和 A 组),以识别质量较差的血管造影。
在 M 和 A 组中,除 M 组中的 vFFR 外,QFR/vFFR 和 FFR 之间均观察到良好的一致性。在 M 组中,fQFR/cQFR/vFFR 与 FFR 之间的相关系数分别为 0.6242、0.5888、0.4089,r 值显著低于 r 值(p=0.0303),而在 A 组中,r 值分别为 0.7055、0.6793、0.5664。在 M 组中,检测 FFR≤0.80 的病变的 AUC 分别为 0.852(95%CI 0.722-0.913)、0.858(95%CI 0.778-0.917)、0.682(95%CI 0.586-0.768),fQFR/cQFR/vFFR 表现优于 vFFR(p=0.0063)和 cQFR(p=0.0054)。在 A 组中,fQFR/cQFR/vFFR 的 AUC 分别为 0.898(95%CI 0.811-0.945)、0.892(95%CI 0.803-0.949)、0.843(95%CI 0.746-0.914)。在 A 组中,AUC 明显高于 M 组(p=0.0399)。
在 7.5fps 和 7pps 血管造影下,QFR/vFFR 评估是可行的,cQFR 与 fQFR 相比没有优势。我们新开发的算法排除方法可能是一种更好的选择血管造影方法,以获得足够质量的血管造影衍生的 FFR 评估。