Department of Gastroenterology, Ichikawa General Hospital, Tokyo Dental College, 5-11-13 Sugano, Ichikawa, Chiba, 272-8513, Japan.
Department of Pathology and Laboratory Medicine, Ichikawa General Hospital, Tokyo Dental College, Ichikawa, Chiba, Japan.
Sci Rep. 2022 Mar 10;12(1):4202. doi: 10.1038/s41598-022-07947-1.
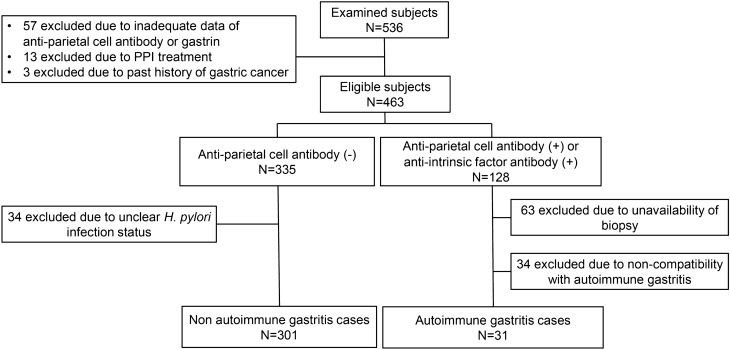
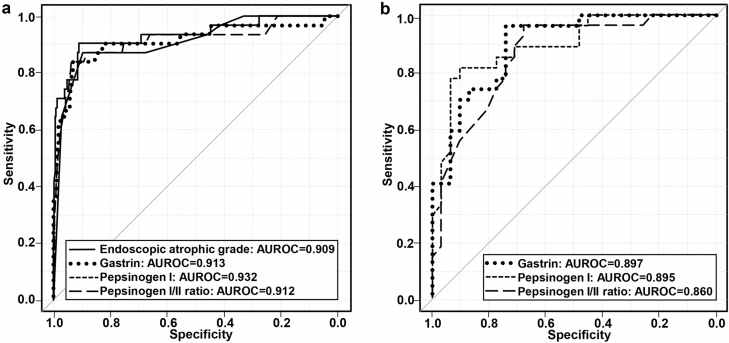
Simple objective modalities are required for evaluating suspected autoimmune gastritis (AIG). This cross-sectional study aimed to examine whether pepsinogen, gastrin, and endoscopic findings can predict AIG. The diagnostic performance of endoscopic findings and serology in distinguishing AIG was evaluated. AIG was diagnosed in patients (N = 31) with anti-parietal cell antibody and/or intrinsic factor antibody positivity and histological findings consistent with AIG. Non-AIG patients (N = 301) were seronegative for anti-parietal cell antibodies. Receiver operating characteristic curve analysis of the entire cohort (N = 332) identified an endoscopic atrophic grade cutoff point of O3 on the Kimura-Takemoto classification (area under the curve [AUC]: 0.909), while those of pepsinogen-I, I/II ratio, and gastrin were 20.1 ng/mL (AUC: 0.932), 1.8 (AUC: 0.913), and 355 pg/mL (AUC: 0.912), respectively. In severe atrophy cases (≥ O3, N = 58, AIG/control; 27/31), the cutoff values of pepsinogen-I, I/II ratio, and gastrin were 9.8 ng/mL (AUC: 0.895), 1.8 (AUC: 0.86), and 355 pg/mL (AUC: 0.897), respectively. In conclusion, endoscopic atrophy is a predictor of AIG. High serum gastrin and low pepsinogen-I and I/II ratio are predictors even in the case of severe atrophy, suggesting their usefulness when the diagnosis of AIG is difficult or as serological screening tests.
评估疑似自身免疫性胃炎(AIG)需要简单的客观方法。本横断面研究旨在探讨胃蛋白酶原、胃泌素和内镜表现是否可预测 AIG。评估了内镜表现和血清学在鉴别 AIG 中的诊断性能。在抗壁细胞抗体和/或内因子抗体阳性且组织学表现符合 AIG 的患者(N=31)中诊断为 AIG。非 AIG 患者(N=301)抗壁细胞抗体阴性。对整个队列(N=332)的受试者工作特征曲线分析确定了 Kimura-Takemoto 分类的 O3 级内镜萎缩切点(曲线下面积 [AUC]:0.909),而胃蛋白酶原 I、I/II 比值和胃泌素的切点分别为 20.1ng/mL(AUC:0.932)、1.8(AUC:0.913)和 355pg/mL(AUC:0.912)。在严重萎缩病例(≥O3,N=58,AIG/对照;27/31)中,胃蛋白酶原 I、I/II 比值和胃泌素的切点值分别为 9.8ng/mL(AUC:0.895)、1.8(AUC:0.86)和 355pg/mL(AUC:0.897)。总之,内镜萎缩是 AIG 的预测因素。即使在严重萎缩的情况下,血清胃泌素升高和胃蛋白酶原 I 和 I/II 比值降低也是预测因素,表明它们在 AIG 诊断困难或作为血清学筛查试验时有用。