Department of Orthopaedic Surgery, University of California Irvine, Orange.
School of Medicine, University of California Irvine, Irvine.
Clin Spine Surg. 2022 Aug 1;35(7):319-322. doi: 10.1097/BSD.0000000000001307. Epub 2022 Mar 10.
Retrospective radiologic analysis.
The aim was to investigate if lateral flexion-extension radiographs identify additional cases of degenerative cervical spondylolisthesis (DCS) that would be missed by obtaining solely neutral upright radiographs, and determine the reliability of magnetic resonance imaging (MRI) in diagnosis.
DCS and instability can be a cause of neck pain, radiculopathy, and even myelopathy. Standard anteroposterior and lateral radiographs and MRI of the cervical spine will identify most cervical spine pathology, but spondylolisthesis and instability are dynamic issues. Standard imaging may also miss DCS in some cases.
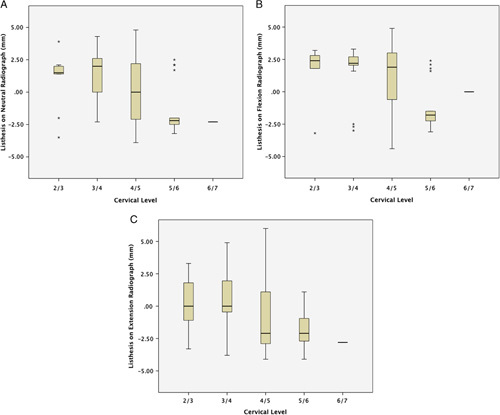
We compared the number of patients who demonstrated cervical spondylolisthesis on lateral neutral and flexion-extension radiographs in addition to MRI. We used established criteria to define instability as ≥2 mm of listhesis on neutral imaging, and ≥1 mm of motion between flexion-extension radiographs.
A total of 111 patients (555 cervical levels) were analyzed. In all, 41 patients (36.9%) demonstrated cervical spondylolisthesis on neutral and/or flexion-extension radiographs. Of the 77 levels of spondylolisthesis, 17 (22.1%) were missed on neutral radiographs ( P ,0.05). Twenty levels (26.0%) were missed when flexion-extension radiographs were used alone ( P =0.02). Twenty-nine levels (37.7%) of DCS identified on radiograph were missed by MRI ( P =0.004).
Lateral flexion-extension views can be useful in the diagnosis of DCS. These views provide value by identifying a significant cohort of patients that would be undiagnosed based on neutral radiographs alone. Moreover, MRI missed 38% of DCS cases identified by radiographs. Therefore, lateral radiographs can be a useful adjunct to neutral radiographs and MRI when instability is suspected or if these imaging modalities are unable to identify the source of a patient's neck or arm pain.
回顾性影像学分析。
旨在探讨侧屈伸展位 X 线片是否能发现单纯中立位 X 线片遗漏的退行性颈椎滑脱(DCS)病例,并确定磁共振成像(MRI)在诊断中的可靠性。
DCS 和不稳定性可能是颈痛、神经根病,甚至是脊髓病的原因。颈椎的标准前后位和侧位 X 线片以及 MRI 可以识别大多数颈椎病变,但滑脱和不稳定是动态问题。在某些情况下,标准影像学检查也可能会遗漏 DCS。
我们比较了在中立位侧位和屈伸位 X 线片以及 MRI 上显示颈椎滑脱的患者数量。我们使用既定标准将≥2mm 的中立位滑脱和屈伸位 X 线片之间≥1mm 的运动定义为不稳定。
共分析了 111 例患者(555 个颈椎节段)。共有 41 例(36.9%)患者在中立位和/或屈伸位 X 线片上显示颈椎滑脱。在 77 个滑脱节段中,17 个(22.1%)在中立位 X 线上漏诊(P<0.05)。单独使用屈伸位 X 线片时漏诊 20 个(26.0%)(P=0.02)。29 个(37.7%)在 X 线片上诊断为 DCS 的病例在 MRI 上漏诊(P=0.004)。
侧屈伸展位 X 线片对 DCS 的诊断有帮助。这些 X 线片通过识别出大量仅基于中立位 X 线片无法诊断的患者,具有重要价值。此外,MRI 漏诊了 38%由 X 线片诊断的 DCS 病例。因此,当怀疑不稳定或这些影像学方法无法确定患者颈痛或臂痛的原因时,侧位 X 线片可以作为中立位 X 线片和 MRI 的有用补充。