Yue Dongsheng, Liu Weiran, Chen Chen, Zhang Tao, Ma Yuchen, Cui Longgang, Gu Yajun, Bei Ting, Zhao Xiaochen, Zhang Bei, Bai Yuezong, Romero Atocha, Xu-Welliver Meng, Wang Changli, Zhang Zhenfa, Zhang Bin
Department of Lung Cancer, Tianjin Lung Cancer Center, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin's Clinical Research Center for Cancer, Tianjin Medical University Cancer Institute and Hospital, Tianjin, China.
Department of Anesthesiology, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin's Clinical Research Center for Cancer, Tianjin Medical University Cancer Institute and Hospital, Tianjin, China.
Transl Lung Cancer Res. 2022 Feb;11(2):263-276. doi: 10.21037/tlcr-22-106.
There is currently a lack of effective biomarkers to evaluate efficacy of neoadjuvant therapy (NAT) for resectable non-small cell lung cancer (NSCLC) patients. Circulating tumor DNA (ctDNA) has been investigated as a non-invasive tool for the assessment of tumor burden and minimal residual disease (MRD). The utility of ctDNA profiling in reflecting NAT efficacy, however, has not been confirmed. This study explored the association of ctDNA change with treatment response to NAT and recurrence-free survival (RFS) after surgery.
Eligible patients with stage IB-IIIA NSCLC were retrospectively included if they had received neoadjuvant immunotherapy combined with chemotherapy (IO+Chemo), dual immunotherapy (IO+IO), or chemotherapy alone (Chemo). We conducted ctDNA profiling before and after NAT, after surgery, and during follow-ups using an ultra-deep lung cancer-specific MRD (LC-MRD) sequencing panel.
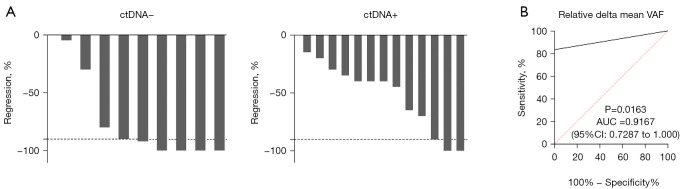
A total of 22 patients who received NAT followed by surgery between August 2018 and July 2019 were included in this study. The major pathological response (MPR) rates were 58.33% (7/12) in the IO+Chemo group, 25.00% (1/4) in the IO+IO group, and 16.67% (1/6) in the Chemo group. The ctDNA dynamics during NAT were highly concordant with pathologic response, demonstrating 100% sensitivity and 83.33% specificity, for an overall accuracy of 91.67%. Pre-surgery detectable ctDNA (after NAT) trended to correlate with inferior RFS [hazard ratio (HR), 7.41; 95% confidence interval (CI): 0.91-60.22, log-rank P=0.03]. At 3-8 days after surgery, ctDNA was detectable in 31.8% of patients and was an independent risk factor for recurrence (HR, 5.37; 95% CI: 1.27-22.67; log-rank P=0.01). The presence of ctDNA at 3 months after surgery showed 83% sensitivity and 90% specificity for predicting relapse (C-index, 0.79; 95% CI: 0.62-0.95). During disease monitoring after surgery, molecular recurrence by means of ctDNA preceded radiographic relapse, with a median time of 6.83 months.
This study investigated the potential of ctDNA in evaluating NAT efficacy in NSCLC, implying the high concordance between ctDNA and pathological response. We also set out the prognostic value of perioperative ctDNA in predicting recurrence.
目前缺乏有效的生物标志物来评估可切除的非小细胞肺癌(NSCLC)患者新辅助治疗(NAT)的疗效。循环肿瘤DNA(ctDNA)已被研究作为一种评估肿瘤负荷和微小残留病(MRD)的非侵入性工具。然而,ctDNA分析在反映NAT疗效方面的实用性尚未得到证实。本研究探讨了ctDNA变化与NAT治疗反应及术后无复发生存期(RFS)之间的关联。
回顾性纳入符合条件的IB-IIIA期NSCLC患者,这些患者接受了新辅助免疫治疗联合化疗(IO+化疗)、双重免疫治疗(IO+IO)或单纯化疗(化疗)。我们使用超深度肺癌特异性MRD(LC-MRD)测序 panel在NAT前后、术后及随访期间进行ctDNA分析。
本研究共纳入了2018年8月至2019年7月期间接受NAT后手术的22例患者。IO+化疗组的主要病理缓解(MPR)率为58.33%(7/12),IO+IO组为25.00%(1/4),化疗组为16.67%(1/6)。NAT期间的ctDNA动态与病理反应高度一致,敏感性为100%,特异性为83.33%,总体准确率为91.67%。术前可检测到的ctDNA(NAT后)与较差的RFS相关[风险比(HR),7.41;95%置信区间(CI):0.91-60.22,对数秩检验P=0.03]。术后3-8天,31.8%的患者可检测到ctDNA,其是复发的独立危险因素(HR,5.37;95%CI:1.27-22.67;对数秩检验P=0.01)。术后3个月ctDNA的存在对预测复发的敏感性为83% ,特异性为90%(C指数,0.79;95%CI:0.62-0.95)。在术后疾病监测期间,通过ctDNA检测到的分子复发先于影像学复发,中位时间为6.83个月。
本研究探讨了ctDNA在评估NSCLC患者NAT疗效方面的潜力,表明ctDNA与病理反应高度一致。我们还阐述了围手术期ctDNA在预测复发方面的预后价值。