Liu Chaoxing, Guo Huaijuan, Mao Haiyan, Tong Jiandong, Yang Mengxue, Yan Xuebing
Department of Oncology, The Affiliated Hospital of Yangzhou University, Yangzhou University, Yangzhou, China.
Department of Oncology, Hefei Cancer Hospital, Chinese Academy of Sciences, Heifei, China.
Front Oncol. 2022 Feb 24;12:753234. doi: 10.3389/fonc.2022.753234. eCollection 2022.
Although immune checkpoint inhibitors (ICIs) have revolutionized the current anticancer therapies, a considerable proportion of patients are found to hardly benefit from these drugs. Accumulating studies have demonstrated that concomitant proton pump inhibitor (PPI) use may affect the clinical efficacy of ICIs; however, their results are inconsistent. In this study, based on updated evidence, we aimed to perform a meta-analysis to clarify the prognostic significance of PPI use in advanced solid cancer patients receiving ICI therapy.
Eligible literature was searched using PubMed, Cochrane Library, Web of Science, EMBASE, and other network resources before July 2021. Clinical outcome was evaluated using overall survival (OS) and progression-free survival (PFS). The correlation of PPI use with OS or PFS was determined based on hazard ratios (HRs) and 95% confidence intervals (CIs).
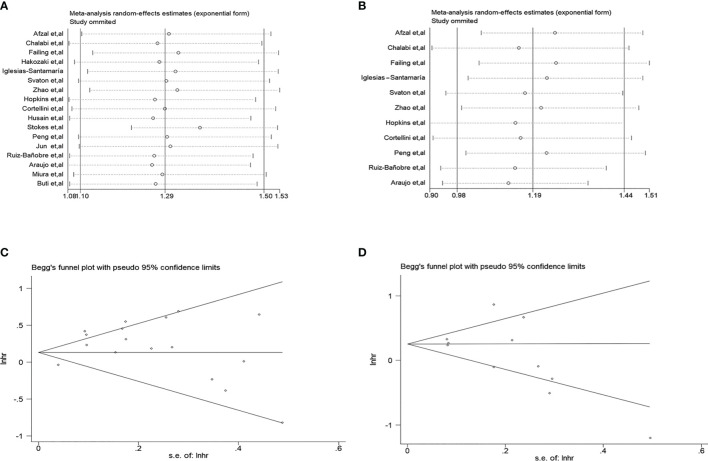
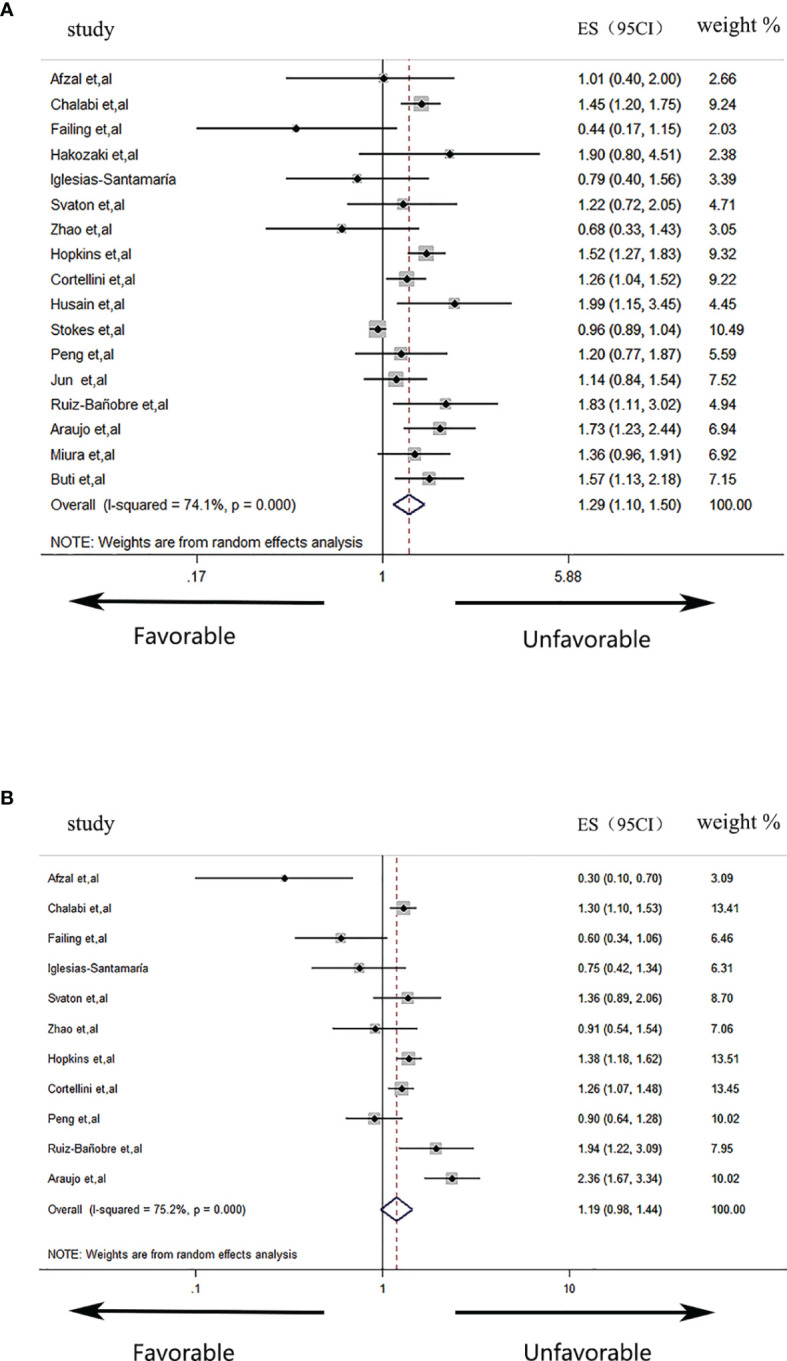
A total of 17 studies enrolling 9,978 ICI-treated cancer patients were included in our meta-analysis. The global analysis demonstrated that PPI use was significantly correlated with worse OS [HR = 1.29 (1.10-1.50)] instead of PFS [HR = 1.19 (0.98-1.44)] in solid cancer patients receiving ICI therapy. In a subgroup analysis, the negative correlation of PPI use with ICI efficacy was significant in patients with non-small cell lung cancer [PFS, HR = 1.27 (1.10-1.47)] and urothelial carcinoma [OS, HR = 1.55 (1.31-1.84), PFS, HR = 1.52 (1.13-2.06)] and mixed cohorts containing multiple cancer types [OS, HR = 1.40 (1.16-1.69)], while an opposite result was observed in the PFS of patients with melanoma [HR = 0.48 (0.25-0.90)]. Moreover, the unfavorable prognostic impact of PPI use was also significant in patients over 65 years old [OS, HR = 1.28 (1.05-1.55), PFS, HR = 1.32 (1.12-1.56)] or those receiving anti-PD-1 [OS, HR = 1.37 (1.04-1.79)] or anti-PD-L1 therapies (OS, HR = 1.49 (1.30-1.69), PFS, HR = 1.34 (1.20-1.50). Finally, PPI use was significantly correlated with a worse prognosis in patients receiving PPIs 30 days before and/or after ICI initiation (OS, HR = 1.38 (1.18-1.62), PFS, HR = 1.23 (1.06-1.43)).
Although our global analysis revealed PPI use was not correlated with the PFS of ICI-treated patients, considering the results of our subgroup analysis, PPIs should be still cautiously used shortly before or during ICI therapy. Furthermore, more clinical validations and related mechanism investigations are of great necessity to clarify the clinical correlation of PPI use with ICI efficacy.
[https://www.crd.york.ac.uk/prospero/], PROSPERO [No. CRD42021243707].
尽管免疫检查点抑制剂(ICI)彻底改变了当前的抗癌治疗方法,但仍有相当一部分患者几乎无法从这些药物中获益。越来越多的研究表明,同时使用质子泵抑制剂(PPI)可能会影响ICI的临床疗效;然而,其结果并不一致。在本研究中,基于最新证据,我们旨在进行一项荟萃分析,以阐明PPI在接受ICI治疗的晚期实体癌患者中的预后意义。
在2021年7月之前,使用PubMed、Cochrane图书馆、Web of Science、EMBASE和其他网络资源搜索符合条件的文献。使用总生存期(OS)和无进展生存期(PFS)评估临床结局。基于风险比(HR)和95%置信区间(CI)确定PPI使用与OS或PFS的相关性。
我们的荟萃分析共纳入了17项研究,涉及9978例接受ICI治疗的癌症患者。全球分析表明,在接受ICI治疗的实体癌患者中,使用PPI与较差的OS显著相关[HR = 1.29(1.10 - 1.50)],而非PFS[HR = 1.19(0.98 - 1.44)]。在亚组分析中,PPI使用与ICI疗效的负相关在非小细胞肺癌患者[PFS,HR = 1.27(1.10 - 1.47)]、尿路上皮癌患者[OS,HR = 1.55(1.31 - 1.84),PFS,HR = 1.52(1.13 - 2.06)]以及包含多种癌症类型的混合队列患者[OS,HR = 1.40(1.16 - 1.69)]中显著,而在黑色素瘤患者的PFS中观察到相反的结果[HR = 0.48(0.25 - 0.90)]。此外,在65岁以上的患者[OS,HR = 1.28(1.05 - 1.55),PFS,HR = 1.32(1.12 - 1.56)]或接受抗PD - 1[OS,HR = 1.37(1.04 - 1.79)]或抗PD - L1治疗的患者(OS,HR = 1.49(1.30 - 1.69),PFS,HR = 1.34(1.20 - 1.50))中,PPI使用的不良预后影响也显著。最后,在ICI开始前和/或后30天内使用PPI的患者中,PPI使用与较差的预后显著相关(OS,HR = 1.38(1.18 - 1.62),PFS,HR = 1.23(1.06 - 1.43))。
尽管我们的全球分析显示PPI使用与接受ICI治疗患者的PFS无关,但考虑到亚组分析的结果,在ICI治疗前或治疗期间仍应谨慎使用PPI。此外,需要更多的临床验证和相关机制研究来阐明PPI使用与ICI疗效的临床相关性。
[https://www.crd.york.ac.uk/prospero/],PROSPERO[编号CRD42021243707]。