Silver Samuel A, Goldstein Stuart L, Harel Ziv, Harvey Andrea, Rompies Elizabeth J, Adhikari Neill K, Acedillo Rey, Jain Arsh K, Richardson Robert, Chan Christopher T, Chertow Glenn M, Bell Chaim M, Wald Ron
Division of Nephrology, St. Michael's Hospital, University of Toronto, Toronto, Canada.
Present Address: 190 King Edward Avenue, Toronto, ON M4C 5J8 Canada.
Can J Kidney Health Dis. 2015 Oct 6;2:36. doi: 10.1186/s40697-015-0071-8. eCollection 2015.
Acute kidney injury (AKI) is an increasingly common problem among hospitalized patients. Patients who survive an AKI-associated hospitalization are at higher risk of de novo and worsening chronic kidney disease, end-stage kidney disease, cardiovascular disease, and death. For hospitalized patients with dialysis-requiring AKI, outpatient follow-up with a nephrologist within 90 days of hospital discharge has been associated with enhanced survival. However, most patients who survive an AKI episode do not receive any follow-up nephrology care. This narrative review describes the experience of two new clinical programs to care for AKI patients after hospital discharge: the Acute Kidney Injury Follow-up Clinic for adults (St. Michael's Hospital and University Health Network, Toronto, Canada) and the AKI Survivor Clinic for children (Cincinnati Children's Hospital, USA).
MEDLINE, PubMed, ISI Web of Science.
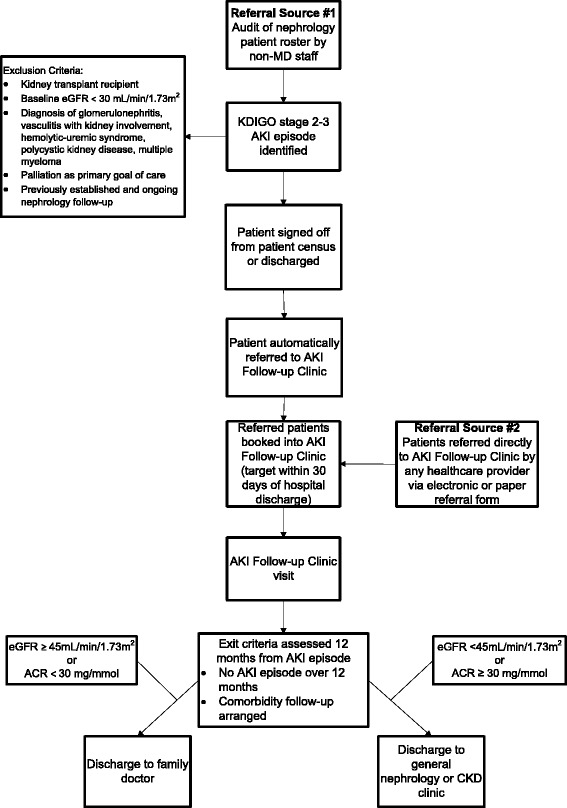
These two ambulatory clinics have been in existence for close to two (adult) and four (pediatric) years, and were developed separately and independently in different populations and health systems. The components of both clinics are described, including the target population, referral process, medical interventions, patient education activities, and follow-up schedule. Common elements include targeting patients with KDIGO stage 2 or 3 AKI, regular audits of the inpatient nephrology census to track eligible patients, medication reconciliation, and education on the long-term consequences of AKI.
Despite the theoretical benefits of post-AKI follow-up and the clinic components described, there is no high quality evidence to prove that the interventions implemented in these clinics will reduce morbidity or mortality. Therefore, we also present a plan to evaluate the adult AKI Follow-up Clinic in order to determine if it can improve clinical outcomes compared to patients with AKI who do not receive follow-up care.
Follow-up of AKI survivors is low, and this review describes two different clinics that care for patients who survive an AKI episode. We believe that sharing the experiences of the AKI Follow-up Clinic and AKI Survivor Clinic provide physicians with a feasible framework to implement their own clinics, which may help AKI patients receive outpatient care commensurate with their high risk status.
急性肾损伤(AKI)在住院患者中是一个日益常见的问题。在与AKI相关的住院治疗中存活下来的患者发生新发和慢性肾脏病恶化、终末期肾病、心血管疾病及死亡的风险更高。对于需要透析的住院AKI患者,出院后90天内由肾病科医生进行门诊随访与生存率提高相关。然而,大多数在AKI发作后存活的患者并未接受任何肾病科的后续护理。这篇叙述性综述描述了两个针对出院后AKI患者的新临床项目的经验:成人急性肾损伤随访诊所(加拿大多伦多圣迈克尔医院和大学健康网络)以及儿童AKI幸存者诊所(美国辛辛那提儿童医院)。
MEDLINE、PubMed、科学引文索引数据库。
这两家门诊诊所分别已运营了近两年(成人诊所)和四年(儿科诊所),它们是在不同人群和卫生系统中分别独立设立的。文中描述了两家诊所的组成部分,包括目标人群、转诊流程、医疗干预、患者教育活动及随访安排。共同要素包括针对KDIGO 2期或3期AKI患者、定期审核住院肾病科普查以追踪符合条件的患者、药物重整以及关于AKI长期后果的教育。
尽管AKI后续随访及所述诊所组成部分在理论上有益,但尚无高质量证据证明这些诊所实施的干预措施会降低发病率或死亡率。因此,我们还提出了一项评估成人AKI随访诊所的计划,以确定与未接受后续护理的AKI患者相比,该诊所是否能改善临床结局。
AKI幸存者的随访率较低,本综述描述了两家为在AKI发作后存活的患者提供护理的不同诊所。我们认为分享AKI随访诊所和AKI幸存者诊所的经验为医生提供了一个可行的框架来建立他们自己的诊所,这可能有助于AKI患者获得与其高风险状况相称的门诊护理。