RRPPS, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Oncology, Birmingham Women's and Children's NHS Foundation Trust, Birmingham, UK.
Pediatr Radiol. 2022 May;52(6):1134-1149. doi: 10.1007/s00247-021-05266-7. Epub 2022 Mar 15.
Relative cerebral blood volume (rCBV) measured using dynamic susceptibility-contrast MRI can differentiate between low- and high-grade pediatric brain tumors. Multicenter studies are required for translation into clinical practice.
We compared leakage-corrected dynamic susceptibility-contrast MRI perfusion parameters acquired at multiple centers in low- and high-grade pediatric brain tumors.
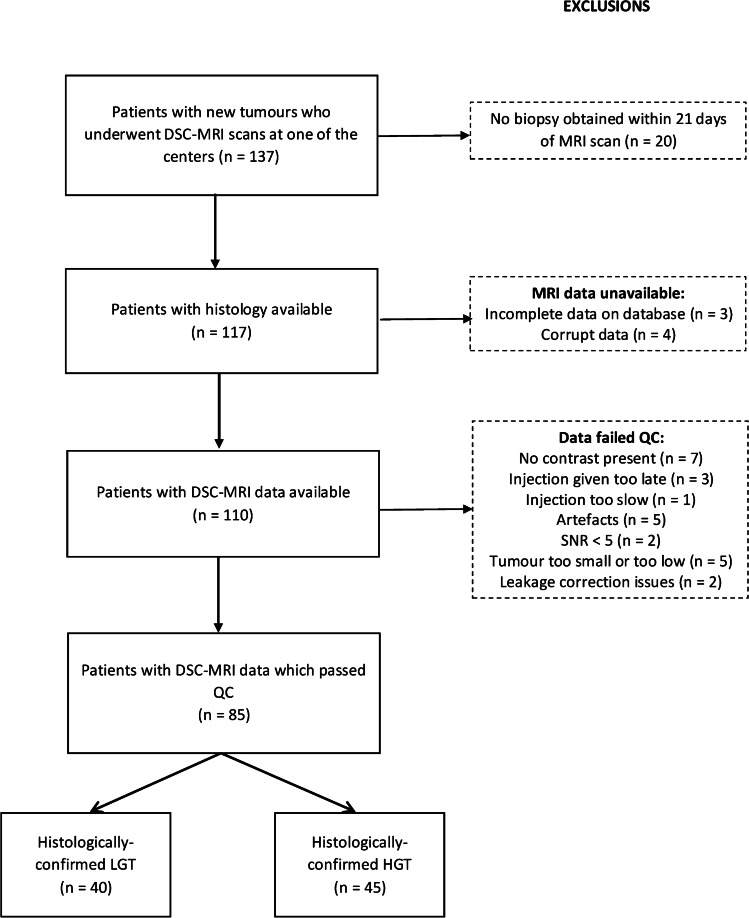
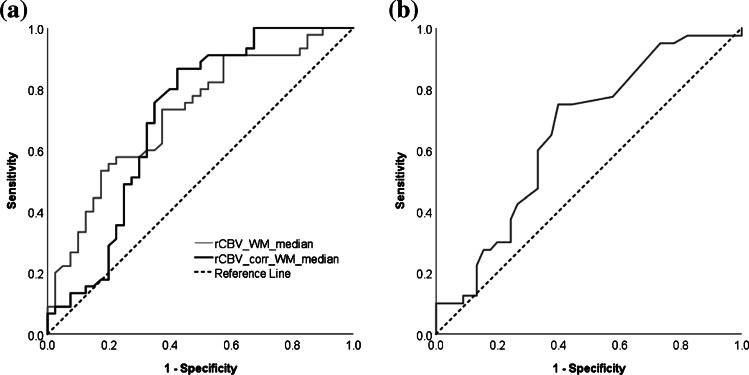
Eighty-five pediatric patients underwent pre-treatment dynamic susceptibility-contrast MRI scans at four centers. MRI protocols were variable. We analyzed data using the Boxerman leakage-correction method producing pixel-by-pixel estimates of leakage-uncorrected (rCBV) and corrected (rCBV) relative cerebral blood volume, and the leakage parameter, K. Histological diagnoses were obtained. Tumors were classified by high-grade tumor. We compared whole-tumor median perfusion parameters between low- and high-grade tumors and across tumor types.
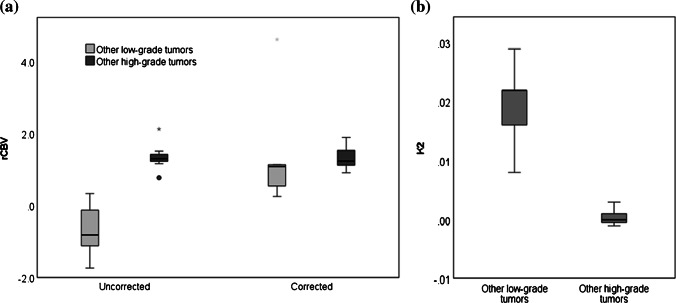
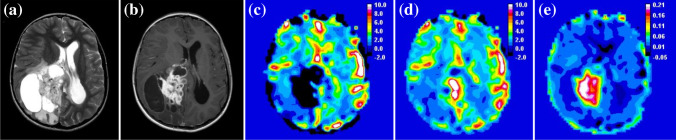
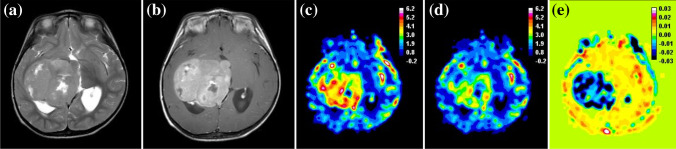
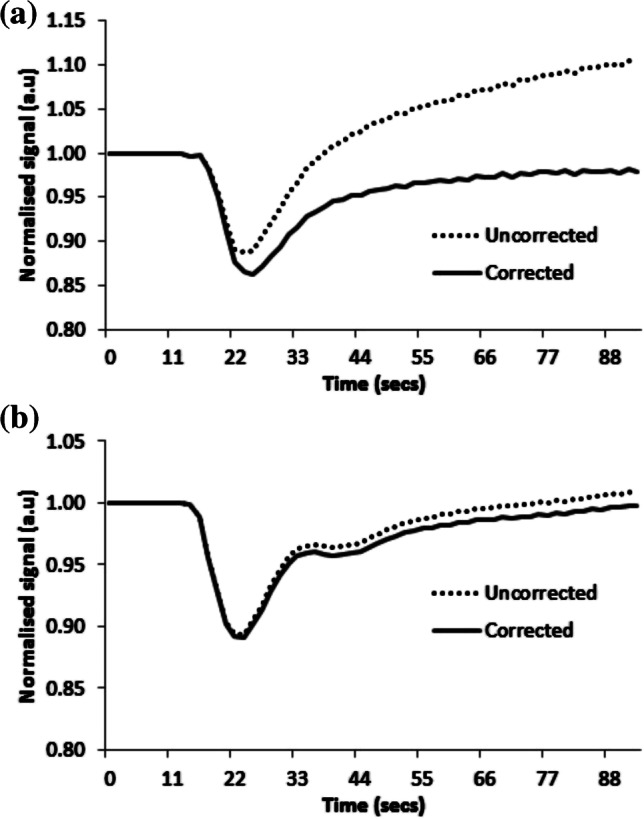
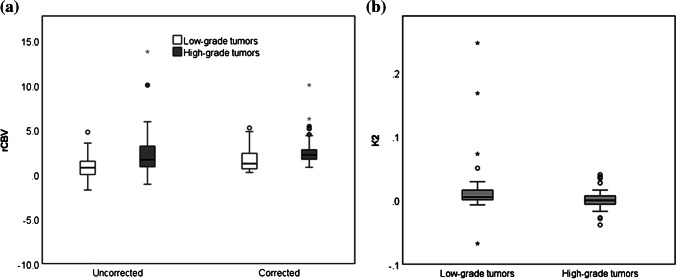
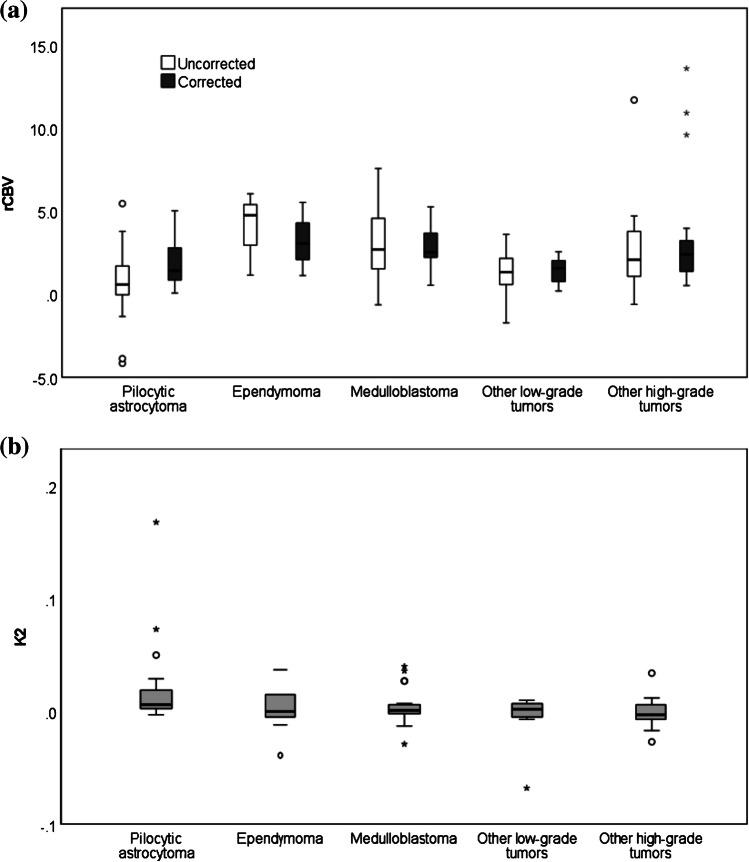
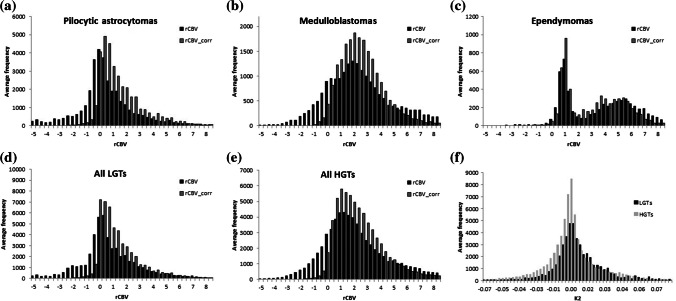
Forty tumors were classified as low grade, 45 as high grade. Mean whole-tumor median rCBV was higher in high-grade tumors than low-grade tumors (mean ± standard deviation [SD] = 2.37±2.61 vs. -0.14±5.55; P<0.01). Average median rCBV increased following leakage correction (2.54±1.63 vs. 1.68±1.36; P=0.010), remaining higher in high-grade tumors than low grade-tumors. Low-grade tumors, particularly pilocytic astrocytomas, showed T1-dominant leakage effects; high-grade tumors showed T2*-dominance (mean K=0.017±0.049 vs. 0.002±0.017). Parameters varied with tumor type but not center. Median rCBV was higher (mean = 1.49 vs. 0.49; P=0.015) and K lower (mean = 0.005 vs. 0.016; P=0.013) in children who received a pre-bolus of contrast agent compared to those who did not. Leakage correction removed the difference.
Dynamic susceptibility-contrast MRI acquired at multiple centers helped distinguish between children's brain tumors. Relative cerebral blood volume was significantly higher in high-grade compared to low-grade tumors and differed among common tumor types. Vessel leakage correction is required to provide accurate rCBV, particularly in low-grade enhancing tumors.
使用动态磁敏感对比 MRI 测量的相对脑血容量 (rCBV) 可区分低级别和高级别儿科脑肿瘤。需要进行多中心研究才能将其转化为临床实践。
我们比较了多个中心在低级别和高级别儿科脑肿瘤中采集的漏校正动态磁敏感对比 MRI 灌注参数。
85 名儿科患者在四个中心接受了治疗前的动态磁敏感对比 MRI 扫描。MRI 方案各不相同。我们使用 Boxerman 漏校正方法分析数据,生成漏校正 (rCBV) 和校正 (rCBV) 相对脑血容量以及漏参数 K 的像素级估计值。获得了组织学诊断。肿瘤根据高级别肿瘤进行分类。我们比较了低级别和高级别肿瘤以及不同肿瘤类型的全肿瘤中位灌注参数。
40 个肿瘤被归类为低级别,45 个肿瘤被归类为高级别。高级别肿瘤的全肿瘤中位 rCBV 高于低级别肿瘤(平均值±标准差 [SD] = 2.37±2.61 vs. -0.14±5.55;P<0.01)。校正漏后平均中位 rCBV 升高(2.54±1.63 vs. 1.68±1.36;P=0.010),高级别肿瘤的 rCBV 仍然高于低级别肿瘤。低级别肿瘤,特别是毛细胞星形细胞瘤,表现出 T1 主导的漏效应;高级别肿瘤表现出 T2*-主导(平均 K=0.017±0.049 vs. 0.002±0.017)。参数随肿瘤类型而变化,但与中心无关。与未接受对比剂预注射的儿童相比,接受预注射对比剂的儿童的 rCBV 更高(平均值=1.49 比 0.49;P=0.015),K 值更低(平均值=0.005 比 0.016;P=0.013)。漏校正消除了差异。
多个中心采集的动态磁敏感对比 MRI 有助于区分儿童脑肿瘤。与低级别肿瘤相比,高级别肿瘤的 rCBV 明显更高,并且在常见肿瘤类型之间存在差异。需要进行血管漏校正以提供准确的 rCBV,特别是在低级别增强肿瘤中。