Wang Kai, Zeng Qin, Li Ke-Xun, Wang Yu, Wang Lu, Sun Ming-Wei, Zeng Jun, Jiang Hua
Department of Acute Care Surgery, Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, Chengdu 610000, China.
Department of Reproductive Medicine, Sichuan Provincial Maternity and Child Health Care Hospital, The Affiliated Women's and children's Hospital of Chengdu Medical College, Chengdu 610045, China.
Burns Trauma. 2022 Mar 14;10:tkac004. doi: 10.1093/burnst/tkac004. eCollection 2022.
Microbial dysbiosis in critically ill patients is a leading cause of mortality and septic complications. Probiotics and synbiotics have emerged as novel therapy on gut microbiota to prevent septic complications. However, current evidence on their effects is conflicting. This work aims to systematically review the impact of probiotics or synbiotics in critically ill adult patients.
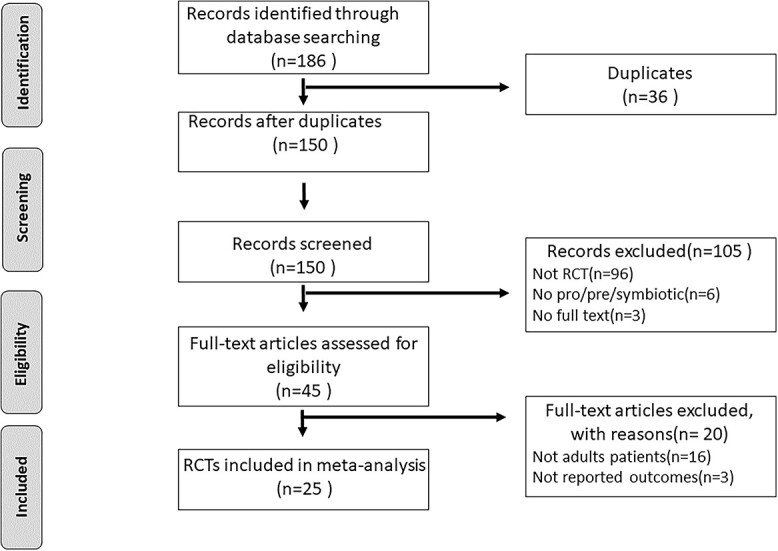
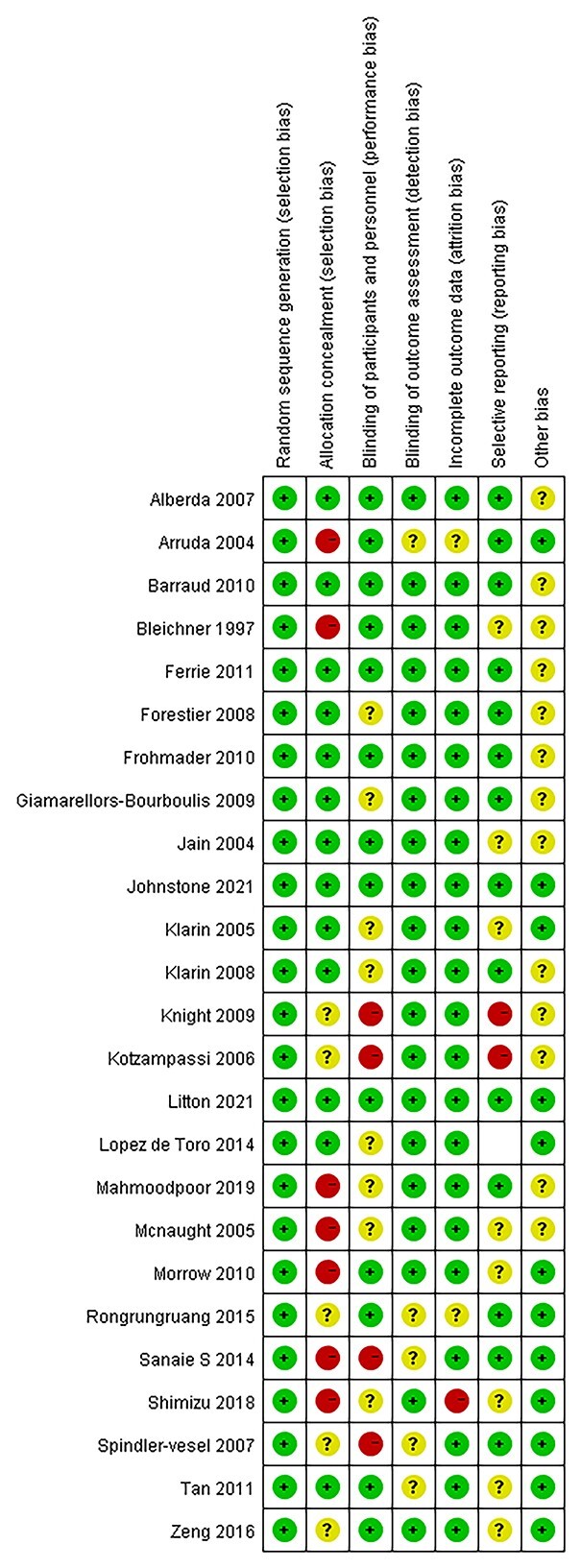
A comprehensive search of the PubMed, CBM, Embase, CENTRAL, ISI, and CNKI databases was performed to identify randomized controlled trials that evaluate probiotics or synbiotics in critically ill patients. The quality assessment was based on the modified Jadad's score scale and the Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1. The major outcome measure was mortality. Secondary outcomes included incidence of septic complications, sepsis incidence, length of intensive care unit (ICU) stay, incidence of non-septic complication, and ventilator day. Data synthesis was conduct by Review Manager 5.4.
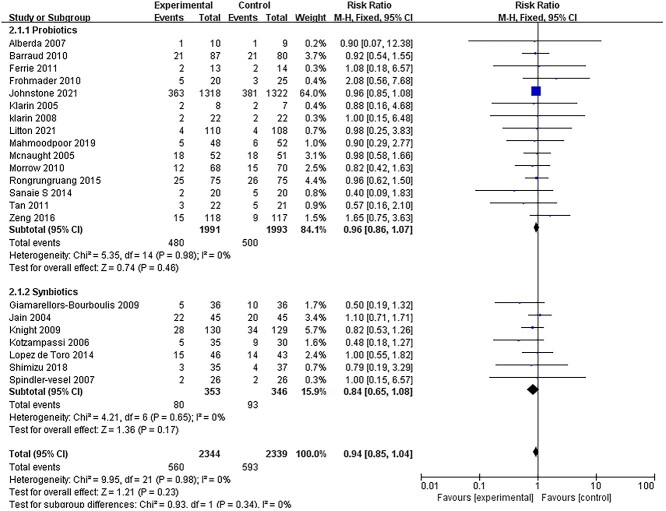
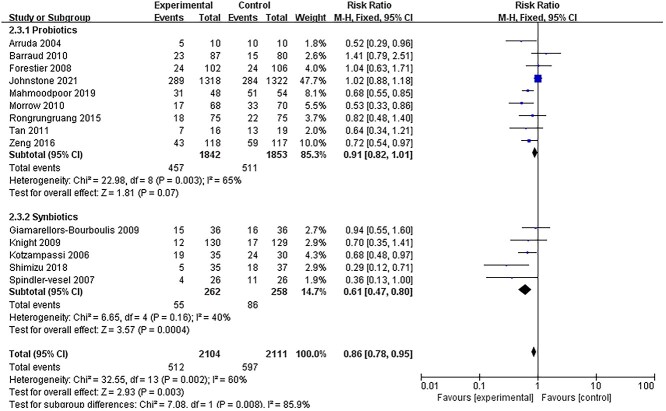
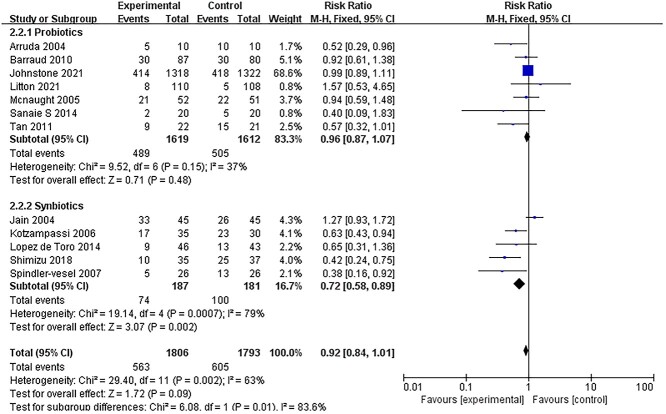
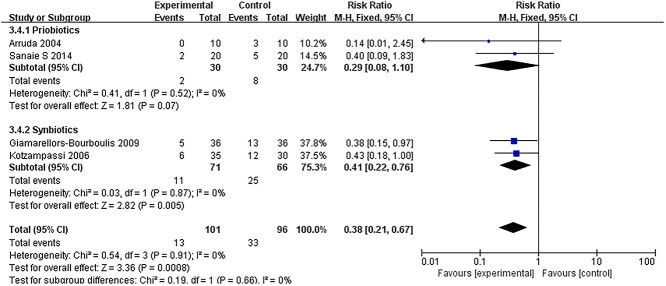
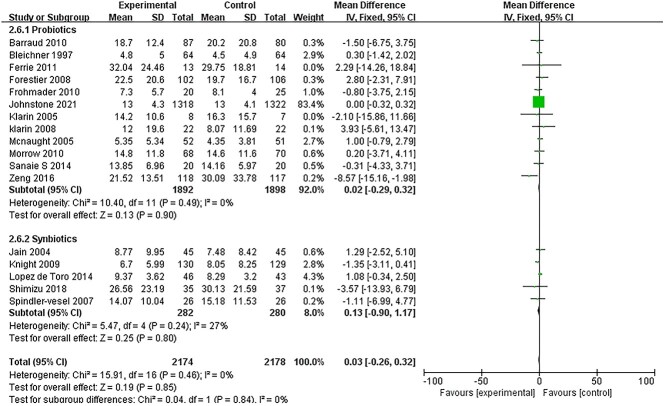
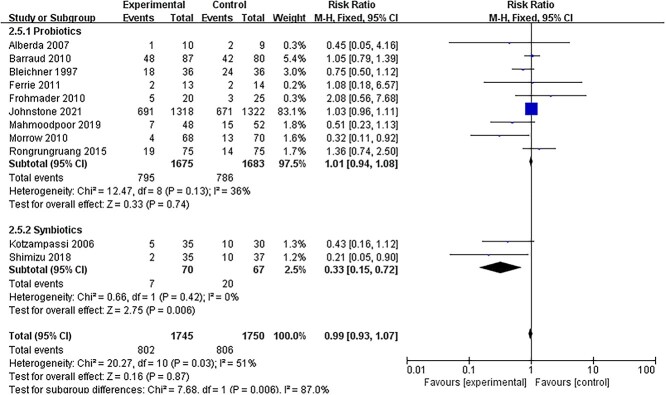
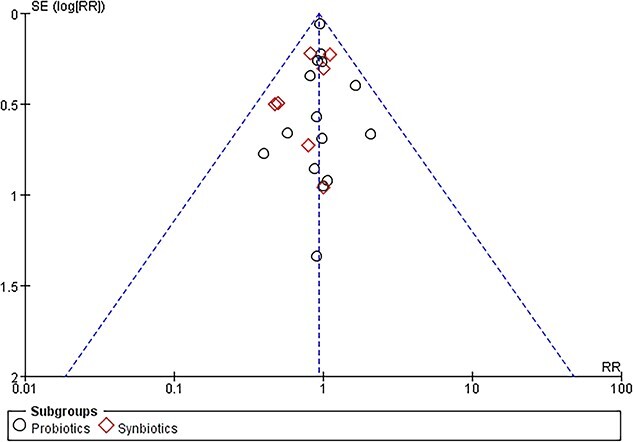
A total of 25 randomized controlled trials reporting on 5049 critically ill patients were included. In the intervention group, 2520 participants received probiotics or synbiotics, whereas 2529 participants received standard care or placebo. Pooling data from randomized controlled trials demonstrated a significant reduction in the incidence of ventilator-associated pneumonia (VAP) in the treatment group [(risk ratio (RR) 0.86; 95% confidence interval (CI): 0.78-0.95; < 0.003, = 85%)]. However, in the subgroup analysis, the reduction of incidence of VAP was only significant in patients receiving synbiotics (RR = 0.61, 95% CI: 0.47-0.80, = 0.0004, = 40%) and not significant in those receiving only probiotics (RR = 0.91, 95% CI: 0.82-1.01, = 0.07, = 65%). Moreover, sepsis incidence of critically ill patients was only significantly reduced by the addition of synbiotics (RR = 0.41; 95% CI: 0.22-0.72, = 0.005, = 0%). The incidence of ICU-acquired infections was significantly reduced by the synbiotics therapy (RR = 0.72; 95% CI: 0.58-0.89, = 0.0007, = 79%). There was no significant difference in mortality, diarrhea, or length of ICU stay between the treatment and control groups.
Synbiotics is an effective and safe nutrition therapy in reducing septic complications in critically ill patients. However, in such patients, administration of probiotics alone compared with placebo resulted in no difference in the septic complications.
危重症患者的微生物群落失调是导致死亡和脓毒症并发症的主要原因。益生菌和合生元已成为调节肠道微生物群以预防脓毒症并发症的新型疗法。然而,目前关于它们作用的证据相互矛盾。这项研究旨在系统评价益生菌或合生元对成年危重症患者的影响。
全面检索PubMed、CBM、Embase、CENTRAL、ISI和CNKI数据库,以识别评估危重症患者使用益生菌或合生元的随机对照试验。质量评估基于改良的Jadad评分量表和《Cochrane系统评价干预措施手册》第5.0.1版。主要结局指标为死亡率。次要结局包括脓毒症并发症的发生率、脓毒症发生率、重症监护病房(ICU)住院时间、非脓毒症并发症的发生率和机械通气天数。采用Review Manager 5.4进行数据合成。
共纳入25项随机对照试验,涉及5049例危重症患者。干预组中,2520名参与者接受了益生菌或合生元,而2529名参与者接受了标准治疗或安慰剂。汇总随机对照试验的数据显示,治疗组呼吸机相关性肺炎(VAP)的发生率显著降低[风险比(RR)0.86;95%置信区间(CI):0.78 - 0.95;P < 0.003,I² = 85%]。然而,在亚组分析中,VAP发生率的降低仅在接受合生元的患者中显著(RR = 0.61,95% CI:0.47 - 0.80,P = 0.0004,I² = 40%),而在仅接受益生菌的患者中不显著(RR = 0.91,95% CI:0.82 - 1.01,P = 0.07,I² = 65%)。此外,仅添加合生元可显著降低危重症患者的脓毒症发生率(RR = 0.41;95% CI:0.22 - 0.72,P = 0.005,I² = 0%)。合生元治疗可显著降低ICU获得性感染的发生率(RR = 0.72;95% CI:0.58 - 0.89,P = 0.0007,I² = 79%)。治疗组和对照组在死亡率、腹泻或ICU住院时间方面无显著差异。
合生元是一种有效且安全的营养疗法,可降低危重症患者的脓毒症并发症。然而,在此类患者中,单独使用益生菌与安慰剂相比,脓毒症并发症并无差异。