Li Cong, Liu Ling, Gao Zhiwei, Zhang Junwei, Chen Hui, Ma Shaolei, Liu Airan, Mo Min, Wu Changde, Chen Dongyu, Liu Songqiao, Xie Jianfeng, Huang Yingzi, Qiu Haibo, Yang Yi
Jiangsu Provincial Key Laboratory of Critical Care Medicine, Department of Critical Care Medicine, School of Medicine, Zhongda Hospital, Southeast University, Nanjing, China.
Department of Critical Care Medicine, School of Medicine, Zhongda Hospital, Southeast University, Nanjing, China.
Front Med (Lausanne). 2021 Jul 15;8:693188. doi: 10.3389/fmed.2021.693188. eCollection 2021.
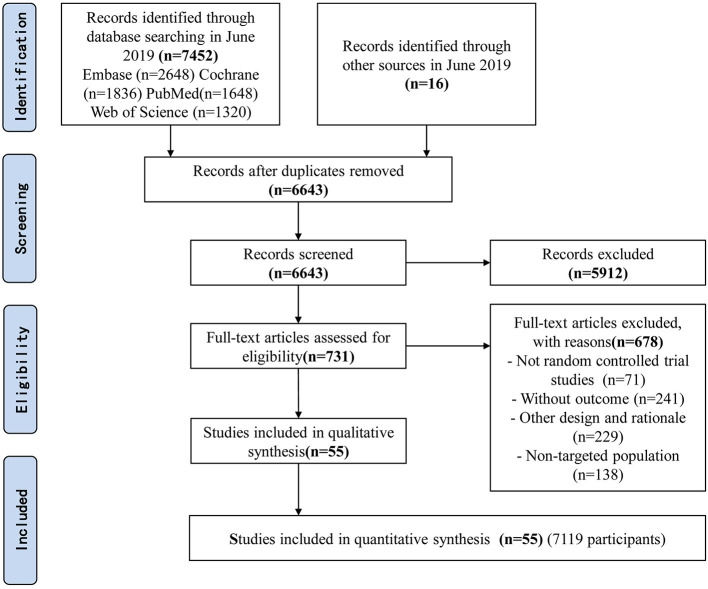
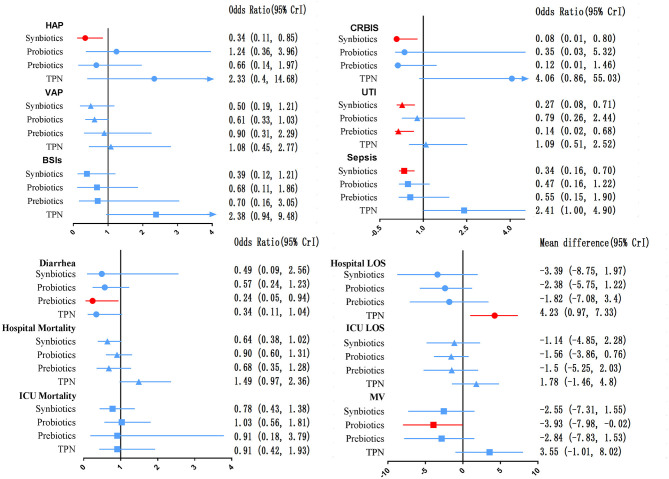
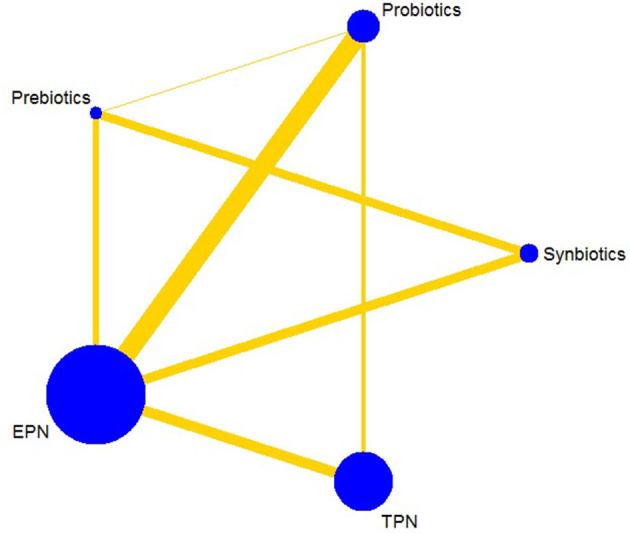
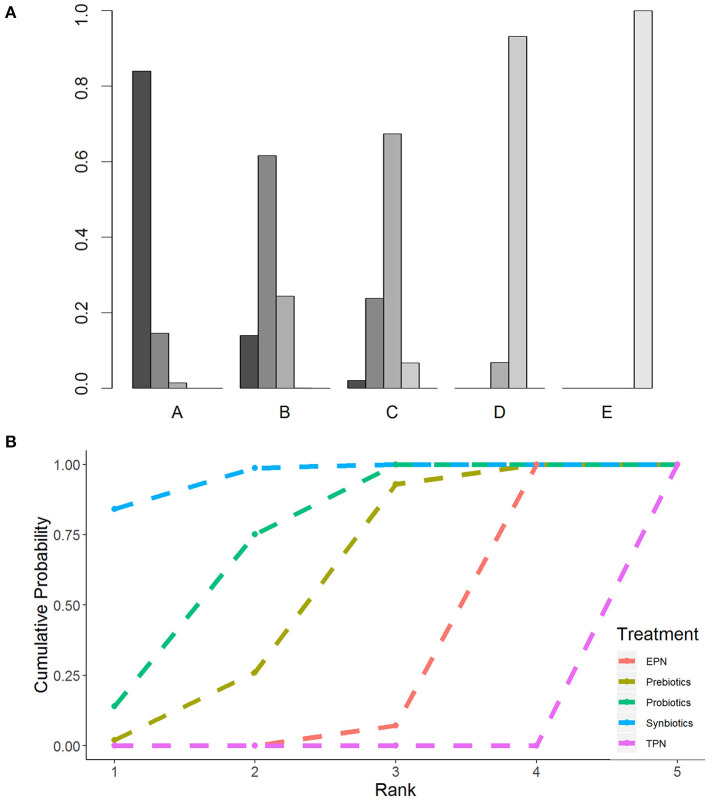
The efficacy of synbiotics, probiotics, prebiotics, enteral nutrition or adjuvant peripheral parenteral nutrition (EPN) and total parenteral nutrition (TPN) in preventing nosocomial infection (NI) in critically ill adults has been questioned. We conducted a systematic review and network meta-analysis (NMA) of randomized controlled trials (RCTs) to evaluate and rank the effectiveness of these therapies on NI amongst critically ill adults. Four electronic databases were systematically searched up to June 30, 2019 for RCTs comparing the administration of probiotics, prebiotics, synbiotics, EPN and TPN in critically ill adults. The primary outcome was NI. The relative efficacy of all outcomes was determined by a Bayesian framework with random effects NMA. We estimated the odds ratio (OR) and mean difference (MD) and ranked the comparative effects of all regimens with the surface under the cumulative ranking probabilities. The study has been registered on PROSPERO (CRD42019147032). Fifty-five RCTs (7,119 patients) were identified. Primary outcome showed that synbiotics had the best effect in preventing NI than EPN (OR 0.37; 95% CrI 0.22-0.61), probiotics followed (OR 0.52; 95% CrI 0.34-0.77), whereas TPN significantly increased NI (OR 2.29; 95% CrI 1.48-3.67). Subgroup analysis showed that TPN significantly increased NI in intensive care unit (ICU) patients (OR 1.57; 95% CrI 1.01-2.56) and severe acute pancreatitis (SAP) patients (OR 3.93; 95% CrI 1.74-9.15). Secondary outcomes showed that synbiotics were more effective in preventing hospital-acquired pneumonia (HAP) (OR 0.34; 95% CrI 0.11-0.85), catheter-related bloodstream infection (OR 0.08; 95% CrI 0.01-0.80), urinary tract infection (OR 0.27; 95% CrI 0.08-0.71) and sepsis (OR 0.34; 95% CrI 0.16-0.70) than EPN. Amongst the treatments, probiotics were most effective for shortening the mechanical ventilation duration (MD -3.93; 95% CrI -7.98 to -0.02), prebiotics were most effective for preventing diarrhea (OR 0.24; 95% CrI 0.05-0.94) and TPN was the least effective in shortening hospital length of stay (MD 4.23; 95% CrI 0.97-7.33). Amongst the five therapies, synbiotics not only prevented NI in critically ill adults but also demonstrated the best treatment results. By contrast, TPN did not prevent NI and ranked last, especially in ICU and SAP patients. Nosocomial infection is a leading cause of mortality in critically ill patients in the ICU. However, the efficacy of synbiotics, probiotics, prebiotics, enteral nutrition or adjuvant peripheral parenteral nutrition and total parenteral nutrition in preventing nosocomial infection in critically ill adults has been questioned. The network meta-analysis provides evidence that amongst the five therapies, synbiotics not only prevented NI in critically ill adults but also demonstrated the best treatment results. By contrast, TPN did not prevent NI and ranked last, especially in ICU and SAP patients. The results of this study will provide a new scientific basis and a new idea for the debate on the efficacy of synbiotics and other treatments in the improvement of prognosis in critically ill adult patients. Synbiotic prevents nosocomial infection in critically ill adults, while total parenteral nutrition has the adverse curative.
合生元、益生菌、益生元、肠内营养或辅助性外周肠外营养(EPN)以及全肠外营养(TPN)在预防危重症成年患者医院感染(NI)方面的疗效受到质疑。我们对随机对照试验(RCT)进行了系统评价和网状Meta分析(NMA),以评估和排序这些疗法对危重症成年患者NI的有效性。系统检索了四个电子数据库,截至2019年6月30日,查找比较益生菌、益生元、合生元、EPN和TPN在危重症成年患者中应用的RCT。主要结局是NI。所有结局的相对疗效通过具有随机效应NMA的贝叶斯框架确定。我们估计了比值比(OR)和均值差(MD),并通过累积排序概率曲线下面积对所有方案的比较效果进行排序。该研究已在PROSPERO(CRD42019147032)注册。共纳入55项RCT(7119例患者)。主要结局显示,合生元在预防NI方面比EPN效果最佳(OR 0.37;95% CrI 0.22 - 0.61),其次是益生菌(OR 0.52;95% CrI 0.34 - 0.77),而TPN显著增加NI(OR 2.29;95% CrI 1.48 - 3.67)。亚组分析显示,TPN在重症监护病房(ICU)患者(OR 1.57;95% CrI 1.01 - 2.56)和重症急性胰腺炎(SAP)患者(OR 3.93;95% CrI 1.74 - 9.15)中显著增加NI。次要结局显示,合生元在预防医院获得性肺炎(HAP)(OR 0.34;95% CrI 0.11 - 0.85)、导管相关血流感染(OR 0.08;95% CrI 0.01 - 0.80)、尿路感染(OR 0.27;95% CrI 0.08 - 0.71)和脓毒症(OR 0.34;95% CrI 0.16 - 0.70)方面比EPN更有效。在这些治疗中,益生菌在缩短机械通气时间方面最有效(MD -3.93;95% CrI -7.98至-0.02),益生元在预防腹泻方面最有效(OR 0.24;95% CrI 0.05 - 0.94),而TPN在缩短住院时间方面效果最差(MD 4.23;95% CrI 0.97 - 7.33)。在这五种疗法中,合生元不仅能预防危重症成年患者的NI,而且显示出最佳治疗效果。相比之下,TPN不能预防NI且排名最后,尤其是在ICU和SAP患者中。医院感染是ICU中危重症患者死亡的主要原因。然而,合生元、益生菌、益生元、肠内营养或辅助性外周肠外营养以及全肠外营养在预防危重症成年患者医院感染方面的疗效受到质疑。网状Meta分析提供的证据表明,在这五种疗法中,合生元不仅能预防危重症成年患者的NI,而且显示出最佳治疗效果。相比之下,TPN不能预防NI且排名最后,尤其是在ICU和SAP患者中。本研究结果将为关于合生元和其他治疗方法在改善危重症成年患者预后方面疗效的争论提供新的科学依据和新思路。合生元可预防危重症成年患者的医院感染,而全肠外营养具有不良疗效。