Broyles Justin M, Balk Ethan M, Adam Gaelen P, Cao Wangnan, Bhuma Monika Reddy, Mehta Shivani, Dominici Laura S, Pusic Andrea L, Saldanha Ian J
Department of Surgery, Division of Plastic and Reconstructive Surgery, Harvard Medical School, Boston, Mass.
Center for Evidence Synthesis in Health, Department of Health Services, Policy, and Practice, Brown University School of Public Health, Providence, R.I.
Plast Reconstr Surg Glob Open. 2022 Mar 11;10(3):e4180. doi: 10.1097/GOX.0000000000004180. eCollection 2022 Mar.
For women undergoing breast reconstruction after mastectomy, the comparative benefits and harms of implant-based reconstruction (IBR) and autologous reconstruction (AR) are not well known. We performed a systematic review with meta-analysis of IBR versus AR after mastectomy for breast cancer.
We searched Medline, Embase, Cochrane CENTRAL, CINAHL, and ClinicalTrials.gov for studies from inception to March 23, 2021. We assessed the risk of bias of individual studies and strength of evidence (SoE) of our findings using standard methods.
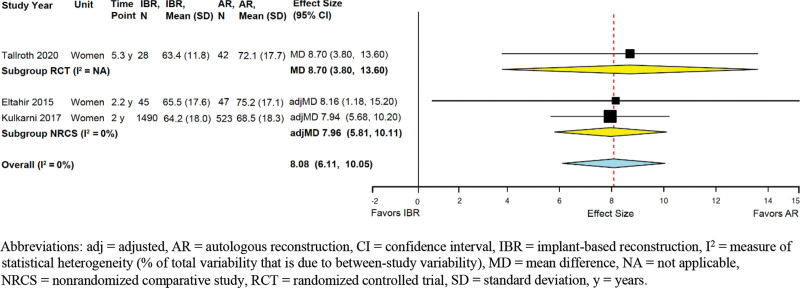
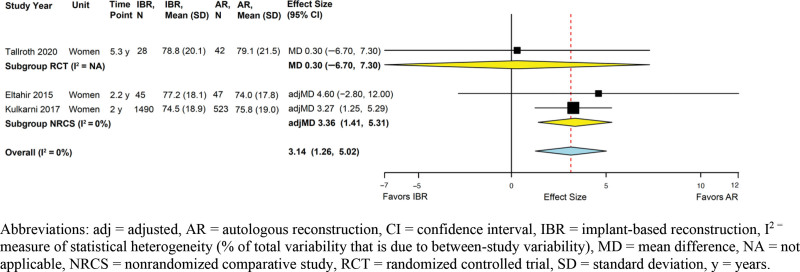
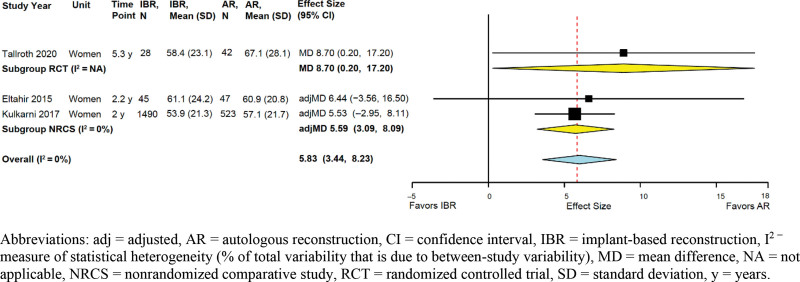
We screened 15,936 citations and included 40 studies (two randomized controlled trials and 38 adjusted nonrandomized comparative studies). Compared with patients who undergo IBR, those who undergo AR experience clinically significant better sexual well-being [summary adjusted mean difference (adjMD) 5.8, 95% CI 3.4-8.2; three studies] and satisfaction with breasts (summary adjMD 8.1, 95% CI 6.1-10.1; three studies) (moderate SoE for both outcomes). AR was associated with a greater risk of venous thromboembolism (moderate SoE), but IBR was associated with a greater risk of reconstructive failure (moderate SoE) and seroma (low SoE) in long-term follow-up (1.5-4 years). Other outcomes were comparable between groups, or the evidence was insufficient to merit conclusions.
Most evidence regarding IBR versus AR is of low or moderate SoE. AR is probably associated with better sexual well-being and satisfaction with breasts and lower risks of seroma and long-term reconstructive failure but a higher risk of thromboembolic events. New high-quality research is needed to address the important research gaps.
对于乳房切除术后进行乳房重建的女性,基于植入物的重建(IBR)和自体组织重建(AR)的相对益处和危害尚不明确。我们对乳腺癌乳房切除术后IBR与AR进行了系统评价和荟萃分析。
我们检索了Medline、Embase、Cochrane CENTRAL、CINAHL和ClinicalTrials.gov,纳入自数据库建立至2021年3月23日的研究。我们采用标准方法评估了个体研究的偏倚风险和研究结果的证据强度(SoE)。
我们筛选了15936篇文献,纳入40项研究(2项随机对照试验和38项调整后的非随机对照研究)。与接受IBR的患者相比,接受AR的患者在临床上具有显著更好的性健康状况[汇总调整后平均差(adjMD)5.8,95%可信区间(CI)3.4-8.2;3项研究]和乳房满意度(汇总adjMD 8.1,95%CI 6.1-10.1;3项研究)(两项结果的SoE均为中等)。AR与静脉血栓栓塞风险增加相关(SoE中等),但在长期随访(1.5-4年)中,IBR与重建失败风险增加(SoE中等)和血清肿风险增加(SoE低)相关。其他结果在两组之间具有可比性,或证据不足以得出结论。
关于IBR与AR的大多数证据的SoE为低或中等。AR可能与更好的性健康状况、乳房满意度以及血清肿和长期重建失败的较低风险相关,但血栓栓塞事件风险较高。需要新的高质量研究来填补重要的研究空白。