Department of Clinical & Experimental Medicine, University of Pisa, Pisa, Italy.
Section of Metabolic Diseases & Diabetes, Azienda Ospedaliero Universitaria Pisana, Pisa, Italy.
Front Endocrinol (Lausanne). 2022 Feb 28;13:847778. doi: 10.3389/fendo.2022.847778. eCollection 2022.
Type 2 diabetes (T2D) is a common comorbidity in people living with HIV (PLWH). Anti-hyperglycemic treatment in PLWH is still a challenge, and no randomized controlled studies using new glucose-lowering agents are currently available.
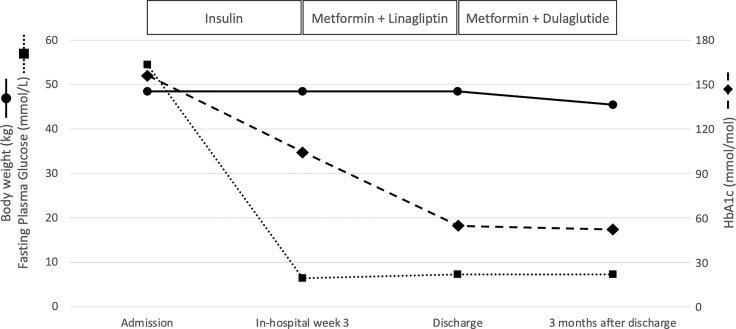
A 55-year-old-women was admitted to our Diabetes Unit because of hyperosmolar hyperglycemic state (HHS) and sepsis. The medical history included HIV infection and insulin-treated diabetes. On clinical examination, the lady appeared dehydrated with dry buccal mucosa, tachycardia, altered mental status, genital infection, and fever. On admission, plasma glucose was 54.5 mmol/L, HbA1c 155 mmol/mol, osmolarity 389.4 mOsm/kg, bicarbonate 24.6 mmol/L with no detectable serum ketones. The patient was treated with i.v. fluid and insulin, and antibiotic therapy commenced. Upon HHS and sepsis resolution, a basal-bolus insulin therapy was implemented that was followed by significant improvement of daily glucose profiles and progressive reduction of insulin requirement until complete discontinuation. A low dose of metformin plus linagliptin was started. Since a severe atherosclerotic disease was diagnosed, a GLP-1 receptor agonist, dulaglutide, was added to metformin upon linagliptin withdrawal with maintenance of good glycemic control, treatment adherence and amelioration of quality of life and no side effects.
This case suggests that GLP-1 receptor agonist therapy may be effective and safe for treatment of T2D with high cardiovascular risk in PLWH, supporting the need of clinical trials directly assessing the safety and the efficacy of GLP-1 receptor agonist in these individuals.
2 型糖尿病(T2D)是 HIV 感染者(PLWH)常见的合并症。PLWH 的抗高血糖治疗仍然是一个挑战,目前尚无使用新型降糖药物的随机对照研究。
一位 55 岁女性因高渗性高血糖状态(HHS)和脓毒症被收入我院糖尿病科。该患者的既往病史包括 HIV 感染和胰岛素治疗的糖尿病。体格检查时,该女士表现为脱水,口腔干燥,心动过速,精神状态改变,生殖器感染和发热。入院时,血浆葡萄糖为 54.5mmol/L,HbA1c 为 155mmol/mol,渗透压为 389.4mOsm/kg,碳酸氢盐为 24.6mmol/L,血清酮体未检出。患者接受了静脉补液和胰岛素治疗,并开始使用抗生素。在 HHS 和脓毒症得到控制后,给予基础-餐时胰岛素治疗,随后每日血糖谱显著改善,胰岛素需求逐渐减少,直至完全停用。开始给予小剂量二甲双胍加利拉鲁肽。由于诊断出严重的动脉粥样硬化性疾病,在停用利拉鲁肽后,加用了 GLP-1 受体激动剂度拉糖肽,同时保持良好的血糖控制、治疗依从性,改善了生活质量,且无不良反应。
本病例提示,GLP-1 受体激动剂治疗可能对合并高心血管风险的 HIV 感染者的 T2D 有效且安全,这支持了在这些人群中直接评估 GLP-1 受体激动剂安全性和疗效的临床试验的必要性。