Centre for Statistics in Medicine, Nuffield Department of Orthopaedics, Rheumatology, and Musculoskeletal Sciences (NDORMS), University of Oxford, Oxford OX3 7LD, UK.
Fundació Institut Universitari per a la recerca a l'Atenció Primària de Salut Jordi Gol i Gurina (IDIAPJGol), Barcelona, Spain.
BMJ. 2022 Mar 16;376:e068373. doi: 10.1136/bmj-2021-068373.
To study the association between covid-19 vaccines, SARS-CoV-2 infection, and risk of immune mediated neurological events.
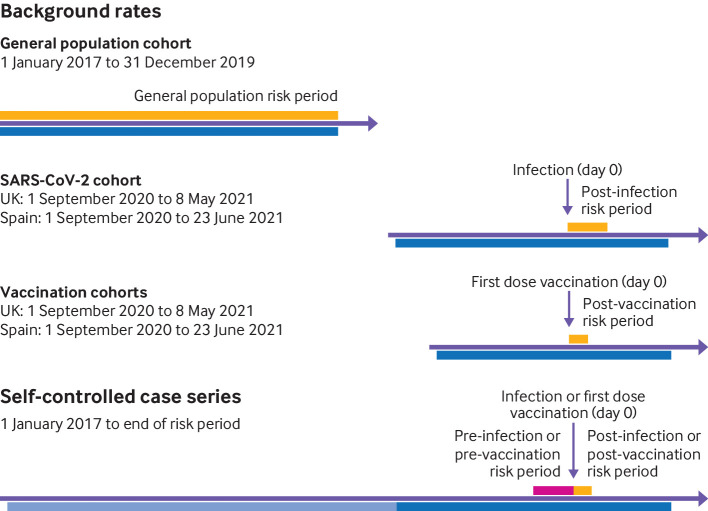
Population based historical rate comparison study and self-controlled case series analysis.
Primary care records from the United Kingdom, and primary care records from Spain linked to hospital data.
8 330 497 people who received at least one dose of covid-19 vaccines ChAdOx1 nCoV-19, BNT162b2, mRNA-1273, or Ad.26.COV2.S between the rollout of the vaccination campaigns and end of data availability (UK: 9 May 2021; Spain: 30 June 2021). The study sample also comprised a cohort of 735 870 unvaccinated individuals with a first positive reverse transcription polymerase chain reaction test result for SARS-CoV-2 from 1 September 2020, and 14 330 080 participants from the general population.
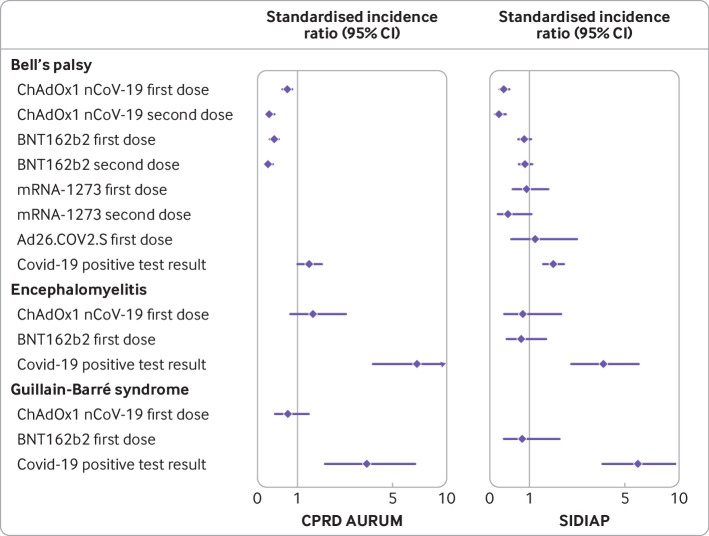
Outcomes were incidence of Bell's palsy, encephalomyelitis, Guillain-Barré syndrome, and transverse myelitis. Incidence rates were estimated in the 21 days after the first vaccine dose, 90 days after a positive test result for SARS-CoV-2, and between 2017 and 2019 for background rates in the general population cohort. Indirectly standardised incidence ratios were estimated. Adjusted incidence rate ratios were estimated from the self-controlled case series.
The study included 4 376 535 people who received ChAdOx1 nCoV-19, 3 588 318 who received BNT162b2, 244 913 who received mRNA-1273, and 120 731 who received Ad26.CoV.2; 735 870 people with SARS-CoV-2 infection; and 14 330 080 people from the general population. Overall, post-vaccine rates were consistent with expected (background) rates for Bell's palsy, encephalomyelitis, and Guillain-Barré syndrome. Self-controlled case series was conducted only for Bell's palsy, given limited statistical power, but with no safety signal seen for those vaccinated. Rates were, however, higher than expected after SARS-CoV-2 infection. For example, in the data from the UK, the standardised incidence ratio for Bell's palsy was 1.33 (1.02 to 1.74), for encephalomyelitis was 6.89 (3.82 to 12.44), and for Guillain-Barré syndrome was 3.53 (1.83 to 6.77). Transverse myelitis was rare (<5 events in all vaccinated cohorts) and could not be analysed.
No safety signal was observed between covid-19 vaccines and the immune mediated neurological events of Bell's palsy, encephalomyelitis, Guillain-Barré syndrome, and transverse myelitis. An increased risk of Bell's palsy, encephalomyelitis, and Guillain-Barré syndrome was, however, observed for people with SARS-CoV-2 infection.
研究 covid-19 疫苗、SARS-CoV-2 感染与免疫介导的神经事件风险之间的关联。
基于人群的历史比率比较研究和自身对照病例系列分析。
来自英国的初级保健记录,以及与医院数据相关联的来自西班牙的初级保健记录。
8330497 人,他们在疫苗接种运动开始到数据可用结束期间(英国:2021 年 5 月 9 日;西班牙:2021 年 6 月 30 日)至少接种了一剂 ChAdOx1 nCoV-19、BNT162b2、mRNA-1273 或 Ad.26.COV2.S 的 covid-19 疫苗。研究样本还包括一组 735870 名未接种疫苗的个体,他们在 2020 年 9 月 1 日之后首次出现 SARS-CoV-2 的逆转录聚合酶链反应检测结果阳性,以及来自一般人群的 14330080 名参与者。
结局为贝尔氏面瘫、脑脊髓炎、格林-巴利综合征和横贯性脊髓炎的发病率。在第一剂疫苗接种后 21 天、SARS-CoV-2 检测结果阳性后 90 天以及 2017 年至 2019 年一般人群队列的背景发病率中估计发病率。间接标准化发病率比进行了估计。从自身对照病例系列中估计了调整后的发病率比。
研究包括 4376535 名接受 ChAdOx1 nCoV-19 接种的人、3588318 名接受 BNT162b2 接种的人、244913 名接受 mRNA-1273 接种的人和 120731 名接受 Ad26.CoV.2 接种的人;735870 名 SARS-CoV-2 感染的人;以及 14330080 名来自一般人群的人。总体而言,疫苗接种后的发生率与贝尔氏面瘫、脑脊髓炎和格林-巴利综合征的预期(背景)发生率一致。仅对贝尔氏面瘫进行了自身对照病例系列研究,因为统计能力有限,但接种疫苗的人群未出现安全信号。然而,在 SARS-CoV-2 感染后,发生率高于预期。例如,在英国的数据中,贝尔氏面瘫的标准化发病率比为 1.33(1.02 至 1.74),脑脊髓炎为 6.89(3.82 至 12.44),格林-巴利综合征为 3.53(1.83 至 6.77)。横贯性脊髓炎很少见(所有接种疫苗队列中<5 例),无法进行分析。
在 covid-19 疫苗与贝尔氏面瘫、脑脊髓炎、格林-巴利综合征和横贯性脊髓炎等免疫介导的神经事件之间未观察到安全信号。然而,对于 SARS-CoV-2 感染的人,观察到贝尔氏面瘫、脑脊髓炎和格林-巴利综合征的风险增加。